Pegloticase FAQ
Answers to common questions about mechanism, applications, research safety, storage, and comparison with rasburicase
Overview
Pegloticase, Recombinant Uricase is a PEGylated recombinant mammalian uric acid oxidase developed for chronic gout in adults who are refractory to conventional therapy. Unlike standard oral gout medications, pegloticase is a biologic enzyme that directly converts uric acid to allantoin, providing a mechanistically distinct route for rapid urate lowering.
This FAQ-style article summarizes the most common questions about pegloticase, including how it works, where it is used, what safety issues matter in research settings, how it should be stored and handled, and how it differs from rasburicase.
pegloticase FAQ, recombinant uricase questions, uricase research uses, gout biologics FAQ, mechanism of action, research safety, rasburicase comparison
1. What Is Pegloticase?
Pegloticase is a PEGylated recombinant uricase enzyme approved for adult patients with chronic gout who have not achieved adequate urate control with conventional therapy or cannot tolerate standard urate-lowering agents. Its active protein is a genetically engineered chimeric uricase incorporating porcine and baboon sequence elements, expressed in Escherichia coli and modified by covalent attachment of monomethoxypoly(ethylene glycol) (mPEG).
PEGylation substantially increases molecular size and extends circulation time, raising the apparent molecular weight from about 136 kDa to roughly 540 kDa. This change reduces rapid elimination and supports an extended half-life of approximately 10 to 14 days.
Pegloticase is supplied as a sterile, preservative-free intravenous formulation. Each vial contains 8 mg in 1 mL of buffered solution and should be stored under refrigeration and protected from light until preparation.
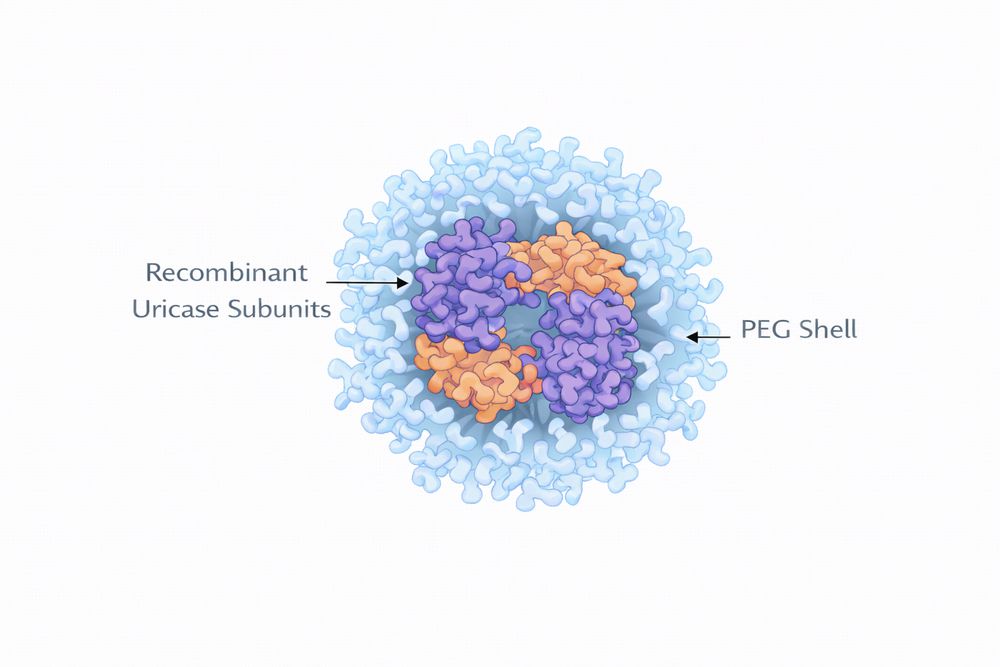
Fig 1. Conceptual structure of PEGylated recombinant uricase.
2. How Does It Work?
Pegloticase catalyzes the oxidation of uric acid to allantoin, a highly soluble end product that humans cannot generate naturally because the human uricase gene is nonfunctional. This creates an extrarenal pathway for uric acid elimination and bypasses the limitations of conventional human metabolism.
2.1 Catalytic Conversion
- Oxidation: uric acid reacts with oxygen to generate 5-hydroxyisourate and hydrogen peroxide.
- Spontaneous downstream conversion: intermediates are converted to allantoin, which is much more soluble than uric acid.
| Property | Uric Acid | Allantoin | Clinical Significance |
|---|---|---|---|
| Molecular weight | 168 Da | 158 Da | Similar size but markedly different physicochemical behavior |
| Water solubility | Poor | Excellent | Allantoin is much easier to excrete |
| Crystal formation | Yes | No | Uric acid drives gout pathology; allantoin does not |
| Physiologic role | Major purine end product in humans | Usually minimal in humans | Pegloticase shifts metabolism toward a more soluble product |
2.2 Pharmacodynamic Effect
After intravenous infusion, serum uric acid may decline within hours. In responders, concentrations can remain below 6 mg/dL for 10 to 14 days, supporting gradual tophus reduction and eventual lowering of flare burden after the early treatment phase.
3. What Is It Used For?
3.1 Clinical Applications
The primary FDA-approved use is chronic gout in adults who are refractory to conventional therapy. This generally includes patients who fail to reach target serum uric acid with maximally tolerated allopurinol or febuxostat, patients who are intolerant to xanthine oxidase inhibitors, or those with relevant contraindications.
- Severe tophaceous gout with disfiguring deposits
- Progressive joint damage despite standard therapy
- Complex gout with comorbid chronic kidney disease or cardiovascular disease
- Preoperative urate debulking when tophi interfere with joint procedures
3.2 Research Applications
| Research Area | Application | Experimental Value |
|---|---|---|
| Purine metabolism | Manipulation of systemic uric acid levels | Supports mechanistic urate biology studies |
| Cardiovascular research | Testing vascular effects of rapid urate lowering | Enables stronger urate reduction than conventional drugs |
| Nephrology | Modeling correction of hyperuricemia in CKD | Useful in renal disease settings |
| Immunology | Characterizing anti-drug antibody responses | Provides a practical model of biologic immunogenicity |
| Drug development | Benchmarking next-generation uricases | Useful PK/PD reference molecule |
| Oxidative stress research | Studying hydrogen peroxide generation | Controlled enzymatic oxidative system |
4. Is It Safe in Research?
The safety of pegloticase in research depends on study format, dose, species, and monitoring intensity. When used appropriately, it is generally manageable in research settings, but the enzymatic reaction and biologic nature of the molecule introduce distinct considerations.
4.1 In Vitro and Tissue Studies
- Generally suitable for cell-based work at controlled concentrations
- Hydrogen peroxide generation may confound oxidative stress endpoints
- Catalase co-treatment may be useful when peroxide is an unwanted variable
- Adequate oxygenation and pH monitoring are important in tissue systems
4.2 Animal and Human Research Settings
| Setting | Key Safety Considerations | Monitoring Parameters |
|---|---|---|
| Cell culture | Hydrogen peroxide-related cytotoxicity | Cell viability and oxidative stress markers |
| Acute animal studies | Rapid urate lowering and immune reactions | Serum urate, hydration, vital observations |
| Chronic animal studies | Immunogenicity and renal follow-up | ADA testing, BUN, creatinine, histology |
| Human research | Infusion reactions and anaphylaxis preparedness | Vital signs, allergic symptoms, emergency support |
Premedication, gradual dose escalation, regular renal and immunologic monitoring, and access to emergency intervention are central elements of safe pegloticase handling in translational or clinical research environments.
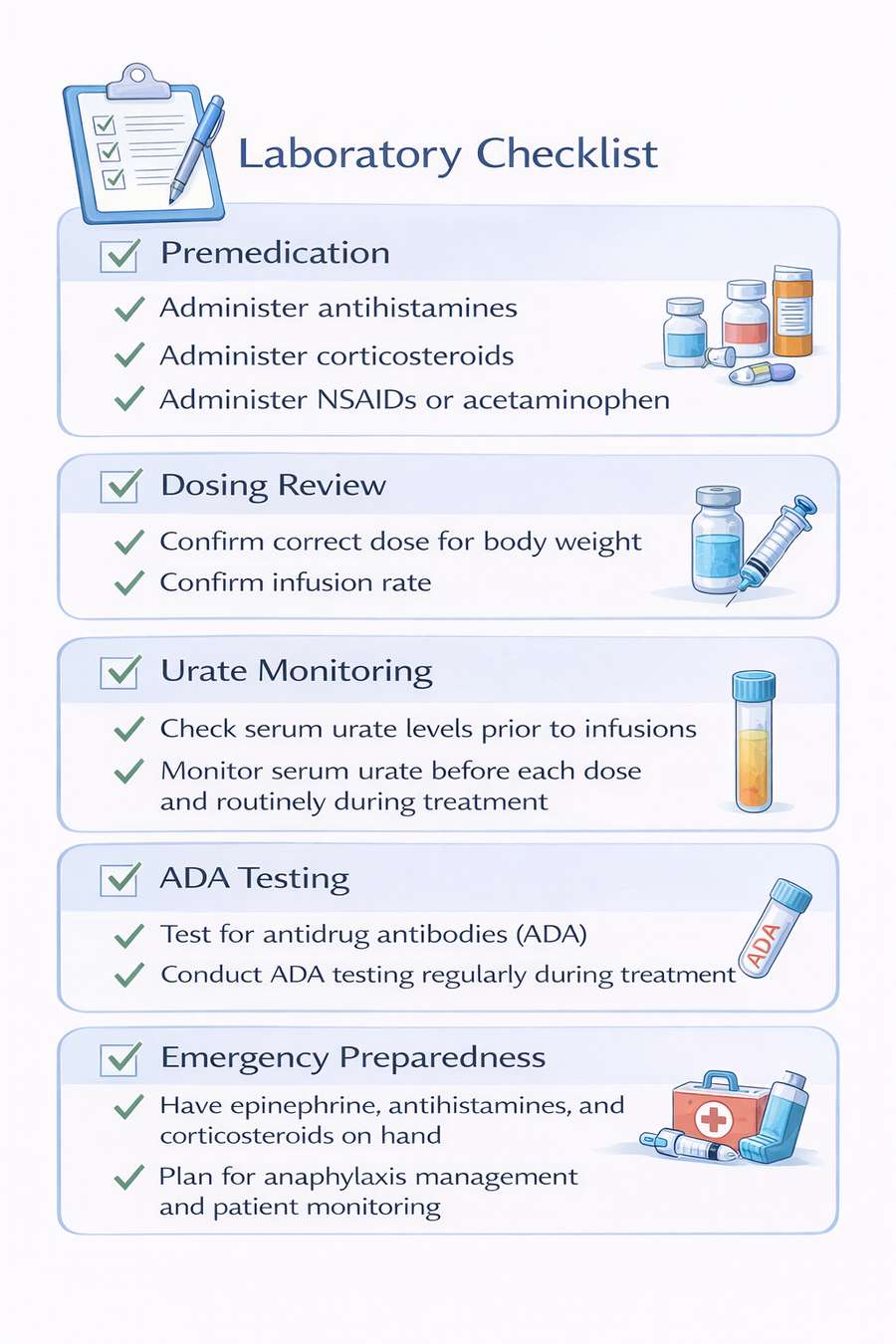
Fig 2. Suggested workflow for pegloticase safety monitoring in research protocols.
5. Storage and Handling
Proper storage and handling are essential for maintaining pegloticase activity and reproducibility. Unopened vials should be refrigerated at 2–8°C, protected from light, and never frozen.
5.1 Preparation Guidance
- Inspect visually before use; solution should be clear and colorless to slightly yellow.
- Dilute using compatible infusion media such as 0.9% sodium chloride or 5% dextrose.
- Mix gently by inversion; do not shake vigorously.
- Use within the recommended post-dilution stability window.
| Condition | Stability | Handling Note |
|---|---|---|
| Unopened vial at 2–8°C | Stable until labeled expiration | Protect from light |
| Diluted solution at room temperature | Approximately 4 hours | Use as soon as possible |
| Diluted solution at 2–8°C | Up to 24 hours | Allow to warm appropriately before administration |
| Frozen material | Not recommended for use | Freezing may denature PEGylated proteins |
6. How Is It Different From Rasburicase?
Both pegloticase and rasburicase are recombinant uricase enzymes, but they differ substantially in source, molecular design, half-life, and use case. Pegloticase is PEGylated and built for chronic refractory gout, whereas rasburicase is a non-PEGylated fungal uricase primarily associated with tumor lysis syndrome settings.
| Feature | Pegloticase | Rasburicase | Implication |
|---|---|---|---|
| Source | Porcine-baboon chimeric mammalian-like uricase | Aspergillus flavus-derived fungal uricase | Different immunogenic profiles |
| PEGylation | Yes | No | Pegloticase has extended half-life and altered exposure profile |
| Molecular weight | Approximately 540 kDa | Approximately 136 kDa | Pegloticase is less susceptible to rapid filtration |
| Terminal half-life | 10–14 days | 18–24 hours | Supports different dosing paradigms |
| Main indication | Chronic refractory gout | Tumor lysis syndrome | Distinct therapeutic contexts |
| Research strength | Sustained urate manipulation and PEG biology | Short-term acute urate lowering | Choice depends on duration and budget needs |
For chronic hyperuricemia studies and PEG-focused biologic research, pegloticase is generally the more relevant model. For shorter and lower-cost screening studies, rasburicase may still be useful.
7. Additional Frequently Asked Questions
Yes. Pegloticase is especially relevant in advanced CKD because it degrades uric acid into allantoin, a more soluble product that is more readily eliminated. In dialysis settings, timing relative to dialysis sessions should be considered.
Rapid urate lowering destabilizes monosodium urate crystal deposits, which can transiently trigger inflammation as deposits begin to dissolve. This is expected and is typically managed with flare prophylaxis.
Oral therapies usually reduce uric acid synthesis or increase excretion. Pegloticase is an intravenous biologic enzyme that directly degrades existing uric acid, enabling deeper and faster urate reduction but requiring infusion-based administration and closer monitoring.
ADA development can accelerate clearance, reduce urate-lowering efficacy, and raise the risk of infusion reactions. This is one of the main reasons therapy may need to be discontinued in non-responders.
Research-grade pegloticase can be used in standard laboratory settings when appropriate handling procedures are in place. Animal work should include proper veterinary support, and cell-based work can usually be performed under standard biosafety and tissue culture practices.
Reports should include source and lot information, dose and route, assay methods for uric acid and allantoin, and any ADA monitoring procedures so results can be interpreted and reproduced accurately.
References
- Becker, M. A., Schumacher, H. R., Wortmann, R. L., et al. Pegloticase in patients with treatment-failure gout. New England Journal of Medicine. 2011;364(11):993-1004.
- Sundy, J. S., Baraf, H. S. B., Yood, R. A., et al. Efficacy and tolerability of pegloticase for the treatment of chronic gout in patients refractory to conventional treatment. JAMA. 2011;306(7):711-720.
- Hershfield, M. S., Ganson, N. J., Kelly, S. J., et al. Induced and pre-existing anti-polyethylene glycol antibody in a trial of every-3-week dosing of pegloticase for refractory gout, including in organ transplant recipients. Arthritis Research & Therapy. 2014;16(2):R63.
- Pui, C. H., Jeha, S., Irwin, D., et al. Recombinant urate oxidase for the prophylaxis or treatment of hyperuricemia in patients with leukemia or lymphoma. Journal of Clinical Oncology. 2001;19(3):697-704.
- Sherman, M. R., Saifer, M. G. P., and Perez-Ruiz, F. PEG-uricase in the management of treatment-resistant gout and hyperuricemia. Advanced Drug Delivery Reviews. 2008;60(1):59-68.