Clinical Evidence Review of Pegloticase in Refractory Gout
A structured review of trial design, efficacy outcomes, safety signals, and future clinical directions
Clinical Background
Chronic refractory gout represents a severe disease state marked by persistent hyperuricemia, recurrent inflammatory flares, progressive tophaceous burden, and substantial loss of quality of life despite optimized conventional therapy. Pegloticase was developed specifically for patients whose disease remains uncontrolled after or intolerant to standard urate-lowering therapies.
The clinical evidence supporting Pegloticase is notable because gout trials combine objective biochemical measures, physical assessments such as tophus burden, and patient-reported outcomes related to pain, function, and health status. Together, these endpoints create a more comprehensive evidence base than serum urate alone.
pegloticase clinical trials, refractory gout treatment, uricase clinical efficacy, biologics gout evidence, study design, efficacy outcomes, safety profile
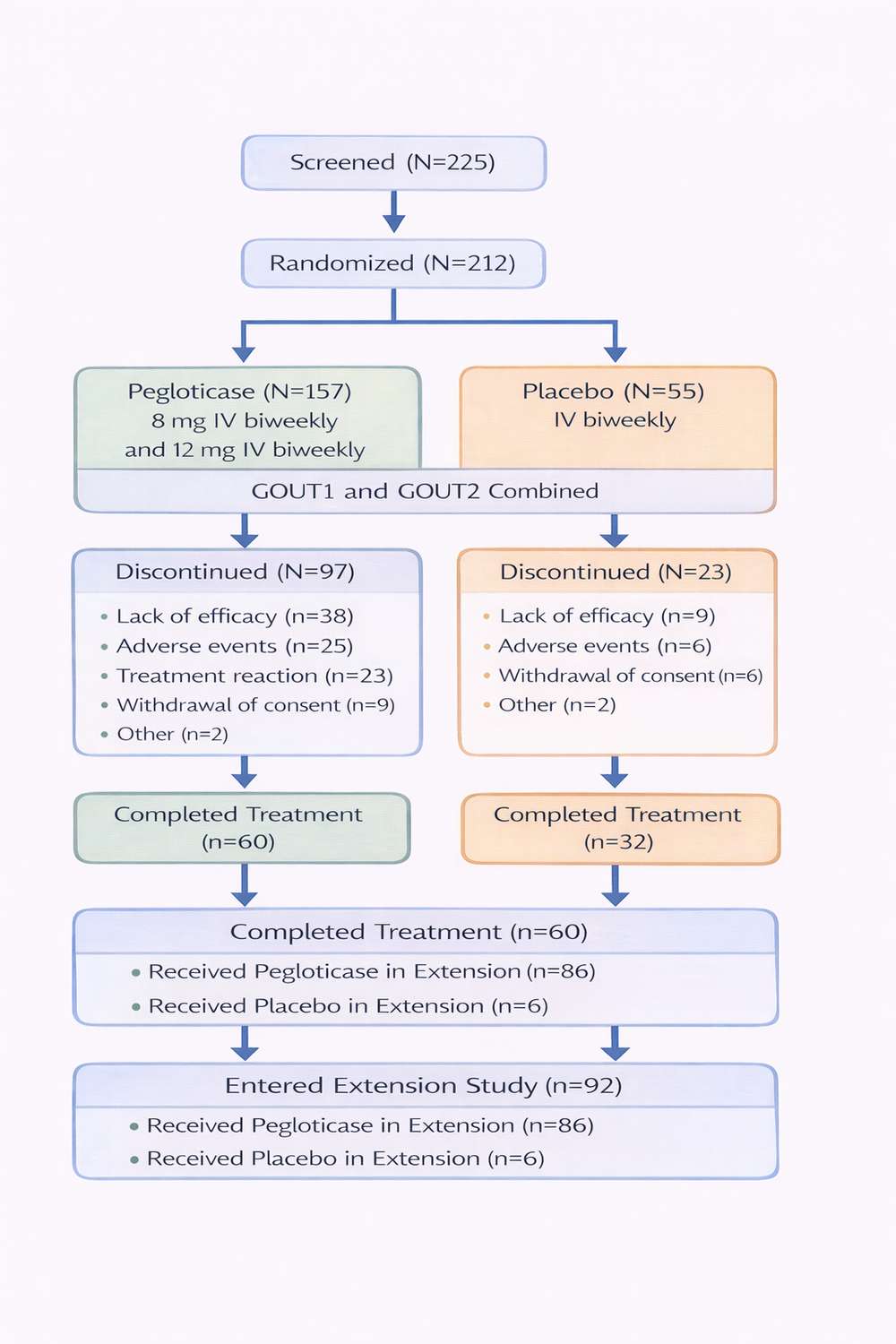
Fig 1. Suggested patient-flow overview for the pivotal clinical program.
1. Study Design
The evidence base for pegloticase includes randomized controlled trials, open-label extension studies, and real-world observational datasets. The two pivotal Phase 3 registration trials, GOUT1 and GOUT2, established the core efficacy and safety profile that supported regulatory approval.
1.1 Pivotal Phase 3 Trial Framework
| Parameter | Specification | Clinical Rationale |
|---|---|---|
| Study population | 225 adults with chronic refractory gout | Focused on patients who failed or could not use conventional urate-lowering therapy |
| Randomization | 2:2:1 (biweekly : monthly : placebo) | Enabled comparison of two active dosing schedules against control |
| Treatment duration | 6 months randomized, followed by open-label extension | Captured both initial and sustained treatment effects |
| Primary endpoint | Plasma uric acid <6 mg/dL for at least 80% of time during months 3-6 | Used an objective biochemical response measure suited to refractory gout |
| Key secondary endpoints | Tophus resolution, flare frequency, HAQ-DI, SF-36 | Integrated clinical, structural, and patient-reported outcomes |
| Premedication | Antihistamine plus corticosteroid | Used to reduce infusion-related reactions |
1.2 Eligibility Criteria
Eligible participants had serum uric acid levels of at least 6 mg/dL despite appropriate prior exposure to allopurinol or febuxostat, or they had intolerance or contraindications to both. Patients also needed meaningful gout burden, such as tophi, recent recurrent flares, or chronic gouty arthritis. Key exclusions included G6PD deficiency, prior severe infusion reactions, uncontrolled cardiovascular disease, and active severe infection.
2. Efficacy Outcomes
The pivotal trials demonstrated that the biweekly regimen delivered the most clinically meaningful and durable response. Results also highlighted an important distinction between short-term urate lowering and sustained responder status over time.
2.1 Primary Endpoint Results
| Treatment Group | Responders | Difference vs. Placebo | P Value |
|---|---|---|---|
| Pegloticase 8 mg biweekly | 47% (47/100) | 47% | <0.001 |
| Pegloticase 8 mg monthly | 20% (12/61) | 20% | 0.04 |
| Placebo | 0% (0/43) | — | — |
The absence of placebo responders underscores how difficult this patient population was to treat with pre-existing approaches. The biweekly schedule clearly outperformed monthly dosing and became the preferred regimen in practice.
2.2 Tophus Resolution and Flare Dynamics
Tophus resolution was one of the most clinically visible benefits. Among biweekly responders, 40% achieved complete resolution of at least one tophus, compared with 7% in the placebo group. Median time to resolution was 13 weeks in biweekly responders.
| Time Period | Biweekly Pegloticase | Placebo | Interpretation |
|---|---|---|---|
| Months 0-3 | 1.15 flares per patient | 0.51 flares per patient | Initial flare increase is expected during rapid urate lowering |
| Months 3-6 | 0.49 flares per patient | 0.64 flares per patient | Flare burden drops as crystal stores dissolve in responders |
| Months 6-12 | 0.30 flares per patient | N/A | Open-label continuation suggests sustained clinical benefit |
2.3 Patient-Reported Outcomes
- HAQ-DI: clinically meaningful reductions of approximately 0.25 to 0.30 points were reported in responders.
- SF-36 Physical Component Summary: improvements of roughly 5 to 7 points supported meaningful gains in physical function.
- Pain VAS: reductions of 20 to 30 mm indicated meaningful symptom relief.
- Patient Global Assessment: marked improvement was reported in approximately 35% to 40% of responders.
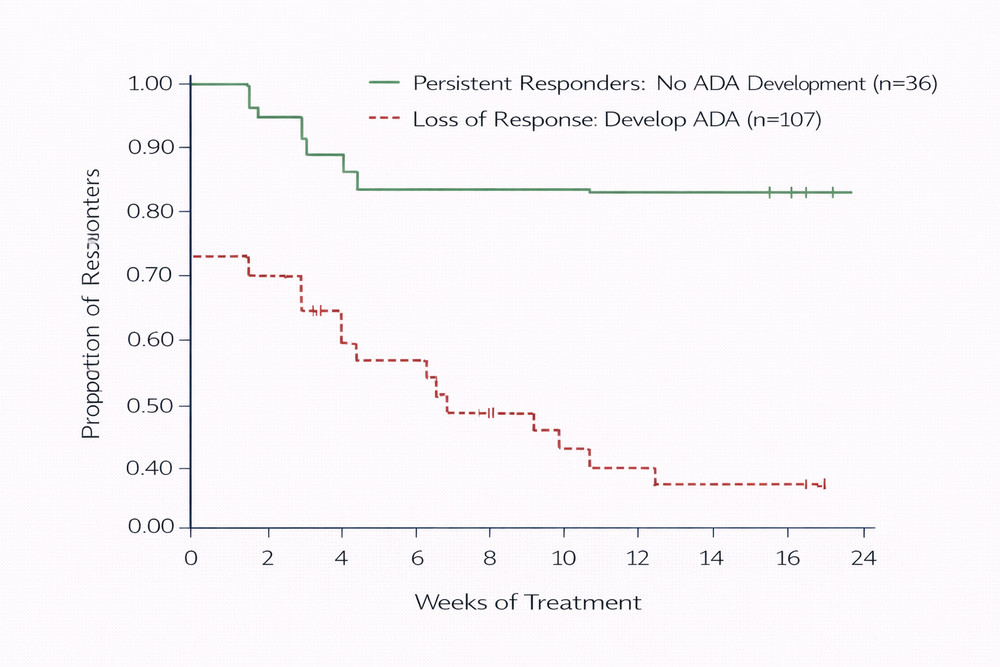
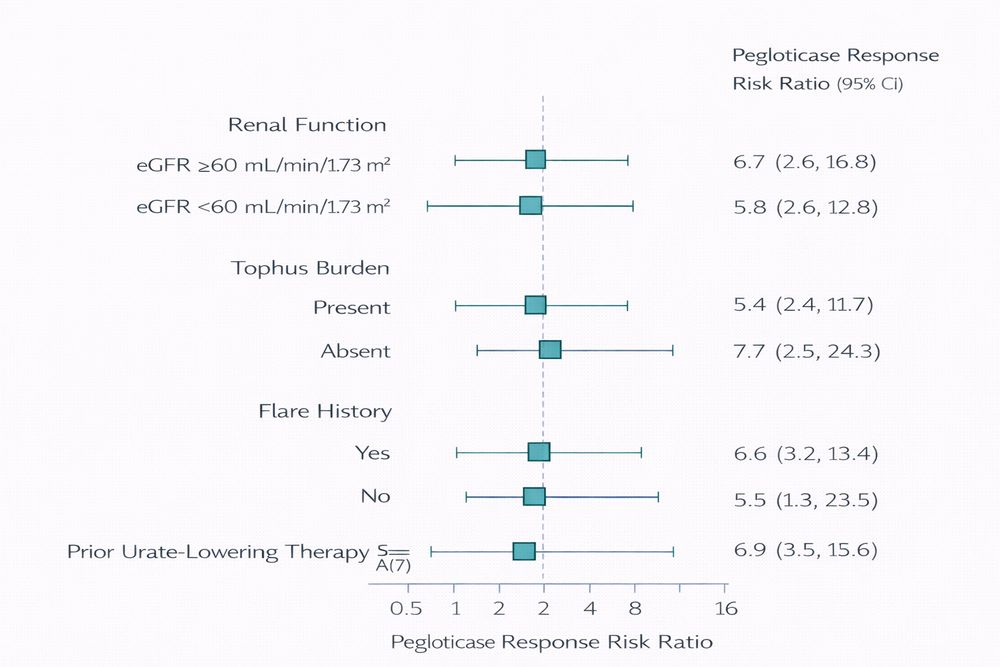
Fig 2-3. Suggested efficacy visuals for treatment durability and subgroup interpretation.
3. Safety Profile
The safety profile of pegloticase reflects its biologic nature, its mechanism of rapid urate depletion, and the central role of immunogenicity in treatment durability. Infusion reactions and gout flares were the most prominent adverse events in the registration program.
| Adverse Event | Biweekly Pegloticase | Monthly Pegloticase | Placebo | Clinical Management |
|---|---|---|---|---|
| Infusion reactions | 26% | 41% | 5% | Premedication, monitoring, and discontinuation if severe |
| Gout flares | 77% | 81% | 53% | Prophylactic colchicine or NSAIDs with breakthrough treatment as needed |
| Nausea | 12% | 20% | 12% | Supportive care |
| Nasopharyngitis | 12% | 10% | 9% | Routine symptomatic management |
| Chest pain | 10% | 10% | 5% | Cardiovascular evaluation when clinically indicated |
| Anaphylaxis | 0% | 2% | 0% | Emergency readiness and permanent discontinuation |
3.1 Infusion Reactions and Immunogenicity
Infusion reactions usually occurred during infusion or within 2 hours after administration and included flushing, urticaria, dyspnea, chest discomfort, hypotension, and, rarely, anaphylaxis. Anti-drug antibodies were detected in most patients, but their clinical consequences varied substantially by titer and neutralizing capacity.
High-titer neutralizing antibodies were strongly associated with loss of urate-lowering response and greater infusion reaction risk. This immunogenicity signal became the dominant limitation in long-term therapy and later motivated immunomodulatory co-therapy strategies.
Pegloticase efficacy can be dramatic in responders, but immunogenicity is the main reason treatment durability fails. Monitoring response trends and infusion tolerance is therefore central to safe use.
4. Real-World Data and Special Populations
Open-label extension studies and post-marketing datasets have broadened the clinical picture beyond the registration trials. In extension studies, approximately 45% of initial responders maintained response at 2 years, with no major new safety signals identified.
4.1 Registry and Observational Findings
- Effectiveness: real-world response rates have generally ranged from 35% to 45%, slightly below trial results but directionally consistent.
- Treatment persistence: median duration has typically been about 5 to 6 months, reflecting immunogenicity and infusion logistics.
- Safety: infusion reaction patterns have been broadly consistent with those observed in controlled trials.
4.2 Special Populations
Organ transplant recipients and patients with chronic kidney disease have received particular attention. In immunosuppressed transplant recipients, lower anti-drug antibody formation and persistent response suggested that background immunosuppression may improve durability. Post-hoc analyses also support efficacy across renal-function strata, including advanced CKD, although dialysis timing remains operationally important.
5. Limitations of the Current Evidence Base
- Immunogenicity-related treatment failure: non-response or loss of response remains the dominant limitation.
- Infusion-based administration: treatment requires healthcare infrastructure and adds logistical burden.
- High treatment cost: reimbursement and access barriers remain important in routine care.
- Limited head-to-head comparison data: placebo-controlled evidence is strong, but comparative effectiveness data remain relatively limited.
These limitations do not undermine the value of pegloticase in appropriately selected refractory patients, but they do define the next wave of optimization efforts in gout biologic therapy.
6. Future Trials and Clinical Direction
Newer studies are addressing the central problem of immunogenicity and exploring whether uricase therapy can become more durable, more convenient, or more broadly usable. The completed MIRROR program demonstrated that methotrexate co-therapy can improve sustained response by reducing immunogenicity. Additional development programs, including next-generation uricase approaches such as SEL-212, aim to further improve clinical persistence.
- Combination strategies with immunomodulation
- More tailored patient selection based on immunogenic risk
- Alternative delivery systems with lower infusion burden
- Broader outcome studies examining cardiovascular and systemic effects of profound urate lowering
References
- Sundy, J. S., Baraf, H. S. B., Yood, R. A., et al. Efficacy and tolerability of pegloticase for the treatment of chronic gout in patients refractory to conventional treatment. JAMA. 2011;306(7):711-720.
- Becker, M. A., Schumacher, H. R., Wortmann, R. L., et al. Pegloticase in patients with treatment-failure gout. New England Journal of Medicine. 2011;364(11):993-1004.
- Botson, J., Peterson, J., and Pretorius, M. Methotrexate to increase response rates in patients with uncontrolled gout receiving pegloticase: MIRROR randomized clinical trial findings. Arthritis & Rheumatology. 2023;75(2):293-304.
- Keenan, R. T., Baraf, H. S. B., LaMoreaux, B., et al. Real-world effectiveness and safety of pegloticase in uncontrolled gout. Seminars in Arthritis and Rheumatism. 2021;51(2):347-352.
- Edwards, N. L. Quality of life and clinical burden in severe refractory gout. Current Rheumatology Reports. 2009;11(2):124-129.