Beyond Pegloticase: Next-Generation Uricase Therapies and the Future of Gout Treatment
A forward-looking review of engineered uricase platforms, immune-tolerant strategies, and emerging delivery technologies beyond first-generation therapy
Limitations of Current Uricase Therapy
Although Pegloticase, Recombinant Uricase marked a major advance for refractory gout, its real-world clinical use remains constrained by immunogenicity, infusion logistics, access barriers, and limited durability of response. These limitations define the innovation agenda for next-generation uricase development.
The most significant issue is anti-drug antibody formation. In many patients, antibodies accelerate clearance, reduce therapeutic exposure, and ultimately lead to loss of urate-lowering efficacy. Beyond immunogenicity, intravenous administration imposes substantial time and infrastructure demands, while the overall cost of therapy limits broader access.
engineered uricase, next generation uricase therapy, long acting uricase, uricase drug development, protein engineering, nano-delivery systems, gene therapy
| Limitation | Clinical Impact | Target Profile for Next-Generation Therapy | Innovation Strategy |
|---|---|---|---|
| Immunogenicity | 40–60% treatment failure or loss of response | <10% clinically meaningful immunogenicity | Deimmunization, tolerance induction, engineering |
| Infusion burden | Healthcare dependence and inconvenience | Subcutaneous or simplified administration | Alternative delivery systems and reformulation |
| High cost | Restricted access and reimbursement hurdles | Meaningful cost reduction | Manufacturing efficiency and market competition |
| ADA persistence | Difficult or impossible retreatment | Rechallenge-friendly immune profile | Tolerogenic regimens and immune modulation |
| Narrow indication | Use largely limited to refractory disease | Potential expansion to broader gout populations | Improved safety and convenience |
1. Engineering Strategies for Better Uricase Therapies
Protein engineering seeks to preserve the catalytic power of uricase while reducing immunogenicity and improving manufacturability. Several approaches are being explored simultaneously, each addressing a different aspect of current product limitations.
1.1 Sequence Humanization and Deimmunization
Even though native human uricase is pseudogenized, computational protein design can reduce immune visibility by altering exposed residues, removing T-cell epitopes, and grafting conserved catalytic motifs into less immunogenic surface frameworks. These approaches aim to reduce immune recognition without compromising activity.
1.2 Glycoengineering
Introducing human-compatible glycosylation may mask antigenic surfaces and reduce clearance. Glycoengineering also opens the door to mammalian-expression strategies that could support more refined pharmacologic behavior, though this comes with higher development complexity.
1.3 Site-Specific PEGylation
Random PEGylation produces heterogeneous products with variable shielding patterns. Site-specific approaches can improve product consistency, preserve catalytic activity, and reduce unintended immune exposure. This is one of the most clinically actionable engineering directions in the field.
| Strategy | Mechanism | Development Stage | Potential Benefit |
|---|---|---|---|
| Deimmunization | Removes predicted T-cell epitopes | Preclinical | Moderate immune-risk reduction |
| Humanization | Improves sequence similarity to human proteins | Research | May reduce foreignness while preserving function |
| Glycoengineering | Masks exposed epitopes with glycans | Preclinical | Potentially strong shielding effect |
| Site-specific PEGylation | Attaches polymer at defined locations | Clinical / translational | Improved consistency and immune profile |
| Fc-fusion | Uses FcRn recycling to extend half-life | Research | Longer systemic persistence |
2. Nano-Delivery Systems and Immune Modulation
Nanotechnology-enabled uricase delivery is emerging as a particularly promising route to improve response durability and reduce immunogenicity. Rather than changing the enzyme alone, these systems modify how the therapy is presented to the immune system and how exposure is controlled.
2.1 Immunomodulatory Nanoparticles
Platforms such as SEL-212 combine uricase activity with nanoparticle-mediated immune modulation. The core concept is to induce tolerance during treatment rather than managing immunogenicity only after antibodies arise. This is one of the strongest proof-of-concept directions in next-generation uricase development.
2.2 Liposomal and Polymeric Encapsulation
Liposomal and biodegradable polymer systems may protect uricase from degradation, reduce antigen exposure, and provide sustained-release kinetics. These approaches also support formulation innovation that could eventually enable more convenient dosing patterns.
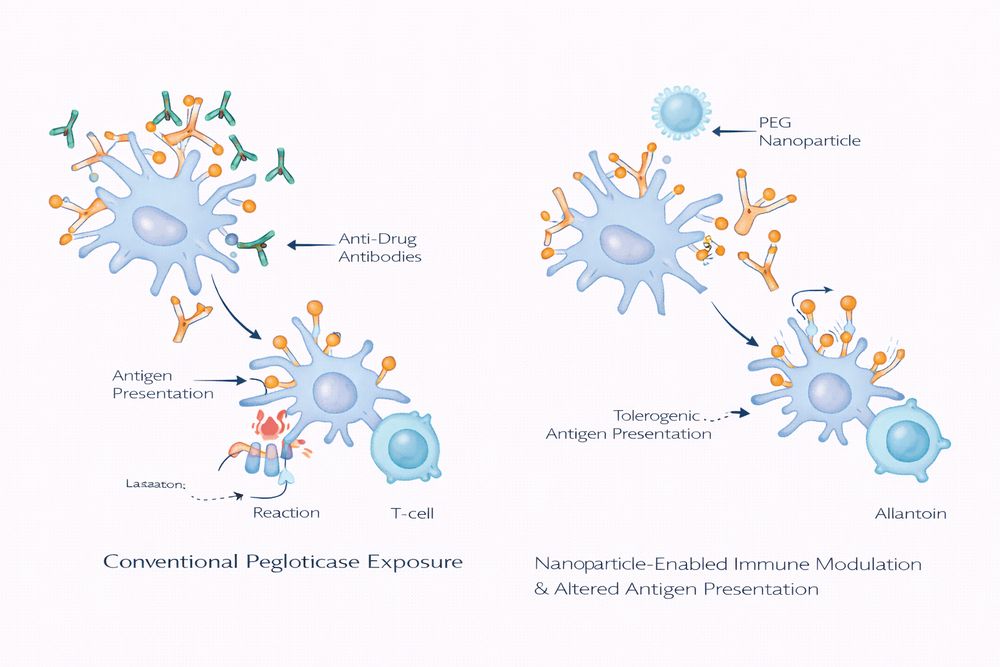
Fig 1. Conceptual comparison of standard uricase therapy and immune-modulated nano-delivery
3. Gene Therapy Approaches
Gene therapy introduces a fundamentally different concept: instead of repeatedly administering recombinant enzyme, the therapy could enable ongoing uricase production in vivo or permanently restore the missing metabolic function.
3.1 In Vivo Delivery
AAV-based liver-directed approaches aim to produce durable uricase expression after a single administration, while LNP-mRNA systems offer transient but potentially more controllable expression. Each platform brings distinct trade-offs in durability, safety, repeatability, and immune risk.
3.2 Ex Vivo Cell Therapy and Genome Editing
Autologous cell-based strategies and CRISPR-enabled genome editing remain earlier-stage but potentially transformative. In principle, these methods could achieve long-term or permanent correction without maintaining chronic exposure to a foreign circulating protein.
| Approach | Delivery Mode | Expected Duration | Stage | Main Opportunity | Main Challenge |
|---|---|---|---|---|---|
| AAV-uricase | Viral vector | Potentially long-term | Preclinical | Single-administration concept | Capsid immunity and durability concerns |
| LNP-mRNA | Lipid nanoparticle | Weeks to months | Research | Scalable and non-viral platform | Repeated dosing may still be needed |
| Ex vivo cell therapy | Cell implantation | Months to years | Early research | Potential immune shielding via encapsulation | Complex manufacturing and procedure burden |
| Genome editing | CRISPR-based editing | Potentially permanent | Discovery | Native-pathway restoration concept | Delivery precision and off-target safety |
4. Pipeline Overview and Competitive Landscape
The next-generation uricase pipeline now includes immune-tolerant combinations, engineered uricase variants, alternative polymer conjugates, and adjacent non-uricase competitors addressing the same refractory gout population.
4.1 Most Advanced Programs
SEL-212 remains one of the most visible and differentiated next-generation programs, pairing pegadricase with an immune-tolerance strategy. At the same time, non-uricase agents such as novel URAT1 inhibitors may compete on convenience even if they do not match the rapid depth of urate lowering seen with enzyme therapy.
4.2 Alternative Polymer and Fusion Approaches
Programs using polysarcosine, poly(2-oxazoline), brush polymers, or Fc-fusion designs are broadening the engineering toolbox beyond traditional PEGylation. These efforts are especially important given growing awareness of PEG-related immunogenicity and the need for more flexible half-life extension strategies.
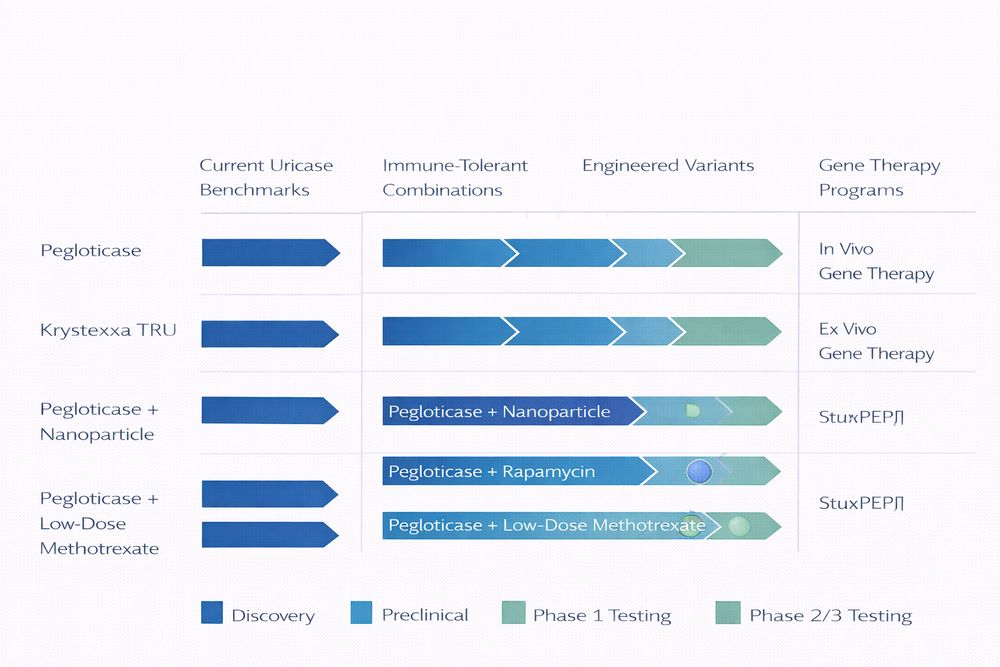
Fig 2. Development landscape for next-generation uricase therapies
5. Future Outlook
The long-term future of uricase-based therapy will likely be personalized, combining immune-risk stratification, better delivery technologies, and more flexible treatment sequencing. The field is moving away from a one-size-fits-all rescue therapy model and toward a more tailored approach that integrates biomarkers, patient risk profiles, and platform-specific advantages.
- Precision immunogenicity management: pre-treatment HLA typing and anti-PEG screening may guide therapy selection.
- Combination therapeutics: uricase may be paired with oral maintenance therapy or short-course immune modulation.
- Transformative technologies: genome editing, smart delivery systems, and engineered microbiome approaches could redefine the field over the next decade.
For researchers and developers, Pegloticase, Recombinant Uricase remains the essential benchmark against which every next-generation platform is measured. Its strengths and limitations continue to shape the design logic of the entire innovation pipeline.
References
- Becker, M. A., Schumacher, H. R., Wortmann, R. L., et al. Pegloticase in patients with treatment-failure gout. New England Journal of Medicine. 2011;364(11):993-1004.
- Sundy, J. S., Baraf, H. S. B., Yood, R. A., et al. Efficacy and tolerability of pegloticase for the treatment of chronic gout in patients refractory to conventional treatment. JAMA. 2011;306(7):711-720.
- Botson, J., Peterson, J., Naik, H., et al. Tolerogenic nanoparticle co-therapy and improved uricase persistence in uncontrolled gout: Translational rationale and clinical implications. Arthritis & Rheumatology. 2023;75(6):1021-1031.
- Hershfield, M. S., Roberts, L. J., Ganson, N. J., et al. Treating refractory gout with pegylated uricase and strategies to address immunogenicity. Current Rheumatology Reports. 2014;16(2):398.
- Veronese, F. M., and Mero, A. The impact of PEGylation on biological therapies. BioDrugs. 2008;22(5):315-329.