Mechanism Comparison of Uricase and Xanthine Oxidase Inhibitors
A translational comparison of enzymatic uric acid degradation and synthesis inhibition in gout management
Overview of Gout Treatments
Gout therapy has progressed from empiric symptom control to mechanism-based intervention, with modern management built around anti-inflammatory agents for acute flares, urate-lowering therapy for long-term disease modification, and biologic enzymes for refractory disease. The current treat-to-target model emphasizes sustained serum urate control below 6 mg/dL, or below 5 mg/dL in tophaceous disease, to promote monosodium urate crystal dissolution and limit progressive joint injury.
Even so, a large fraction of patients do not achieve goal urate levels with first-line oral therapy alone. That gap has driven greater interest in comparing two fundamentally different strategies: xanthine oxidase inhibition, which reduces uric acid production, and uricase-based therapy, which directly degrades circulating uric acid.
uricase vs allopurinol, uric acid metabolism drugs, gout treatment comparison, enzymatic vs inhibition therapy, Pegloticase, patient selection, research implications
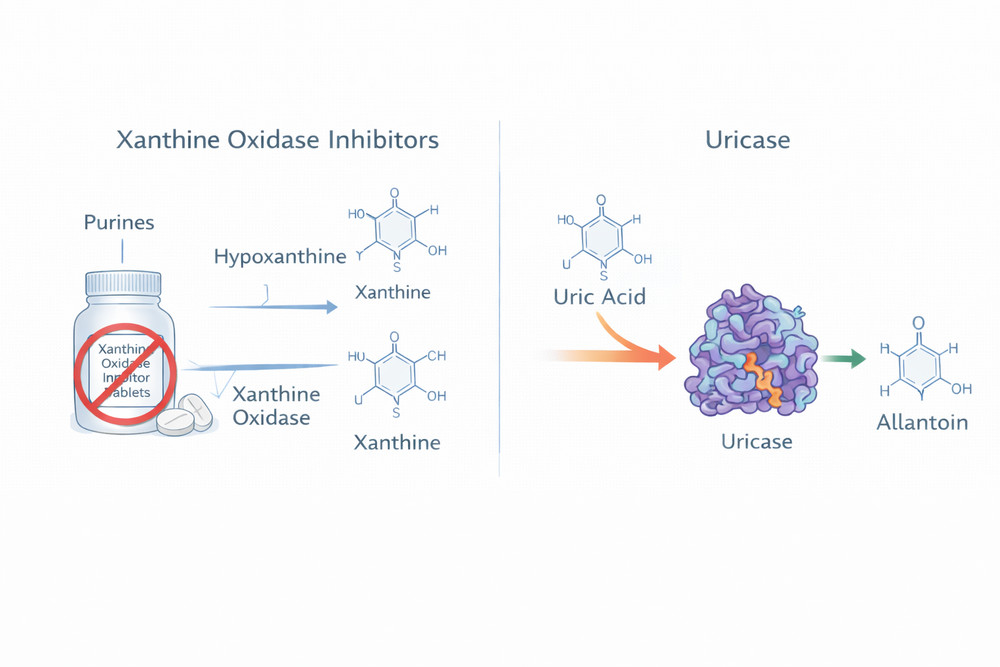
Fig 1. Conceptual comparison of urate-lowering mechanisms
1. Xanthine Oxidase Inhibitors: Blocking Uric Acid Production
Xanthine oxidase inhibitors (XOIs) remain the foundation of chronic gout management. Agents such as allopurinol and febuxostat suppress the final steps of purine catabolism and thereby reduce de novo uric acid synthesis.
1.1 Allopurinol
Allopurinol is a purine analog and hypoxanthine isomer that functions as a mechanism-based inhibitor of xanthine oxidase. After oral administration, it is converted to oxypurinol, which binds tightly to the enzyme and produces durable suppression of uric acid synthesis. In routine clinical use, allopurinol can reduce uric acid production by roughly 60–70% in adherent patients.
1.2 Febuxostat
Febuxostat is a non-purine selective inhibitor that binds reversibly to xanthine oxidase. Because it does not structurally resemble purine substrates, it has a different selectivity profile and generally fewer interactions with other purine pathway enzymes. Its pharmacology can be advantageous in mild-to-moderate renal impairment, although hepatic metabolism remains relevant in patients with liver disease.
1.3 Pharmacologic Comparison of XOIs
| Parameter | Allopurinol | Febuxostat | Mechanistic Implication |
|---|---|---|---|
| Chemical class | Purine analog | Non-purine thiazolecarboxylic acid | Different selectivity and off-target profiles |
| Mechanism | Mechanism-based inhibition via oxypurinol | Competitive, reversible inhibition | Allopurinol may provide longer-lasting enzyme suppression; febuxostat offers a more direct reversible profile |
| Bioavailability | Approximately 80% | Approximately 85% | Both are suitable for oral administration |
| Half-life | 1–3 h parent; 18–30 h oxypurinol | 5–8 h | Metabolite persistence contributes to sustained allopurinol activity |
| Renal considerations | Oxypurinol is renally cleared | Predominantly hepatic metabolism | Allopurinol dose adjustment is often needed in CKD |
| Key safety signal | HLA-B*5801-associated hypersensitivity | Cardiovascular warning in selected populations | Patient stratification remains clinically important |
1.4 Limitations of XOI Therapy
- Pharmacogenetic variability: response and toxicity can vary with genetic background and transporter biology.
- Incomplete efficacy: a meaningful percentage of patients do not reach serum urate targets even after dose optimization.
- Renal dependence: synthesis is reduced, but impaired excretion is not directly corrected.
- Drug interactions: allopurinol in particular requires attention in patients receiving purine analog therapies.
- Hypersensitivity risk: rare but serious reactions can limit long-term use.
2. Uricase Mechanism: Enzymatic Degradation of Existing Uric Acid
Unlike XOIs, Pegloticase and related recombinant uricase strategies do not decrease synthesis upstream. Instead, they catalyze the oxidation of uric acid into allantoin, a highly soluble metabolite that is more readily excreted. This creates a mechanistically distinct pathway that can address both urate overproduction and underexcretion at the same time.
2.1 Enzymatic Degradation Advantages
Because uricase acts on circulating uric acid itself, the onset of serum urate reduction is much faster than with oral inhibition strategies. In responsive patients, profound urate lowering may be observed within 24–48 hours of infusion, and concentrations below 1 mg/dL have been reported in responders. That level of reduction is difficult to replicate with xanthine oxidase inhibition alone.
2.2 Mechanistic Comparison of Urate-Lowering Strategies
| Feature | Xanthine Oxidase Inhibition | Uricase Enzyme Therapy | Clinical Implication |
|---|---|---|---|
| Primary mechanism | Reduce de novo uric acid synthesis | Degrade existing uric acid | Uricase acts on the urate pool already present in circulation |
| Target location | Primarily hepatic enzyme inhibition | Systemic action on plasma urate | Rapid systemic urate clearance is possible with uricase |
| Onset of action | Days to weeks | Hours to 48 hours | Uricase is more suitable when rapid reduction is needed |
| Magnitude of urate lowering | Moderate | Profound | Sub-saturation urate levels are more readily achieved with uricase |
| Renal function dependence | Moderate | Lower | Useful distinction in advanced CKD |
| Administration | Oral daily dosing | Intravenous intermittent dosing | Convenience favors XOIs; potency favors uricase in selected cases |
| Immunogenicity | Not a major issue | Major treatment-limiting concern | Durability of response remains a central challenge for uricase therapy |
2.3 Pharmacokinetic Considerations
PEGylation extends the circulation time of pegloticase and supports biweekly or monthly scheduling, depending on formulation strategy and clinical context. This intermittent dosing pattern may improve adherence for some patients, but the need for infusion-based delivery and monitoring offsets that advantage in routine care.
3. Comparative Efficacy and Safety
3.1 Comparative Efficacy
Direct head-to-head trials are limited because XOIs and uricase therapies are often used in different patient populations. Even so, several practical distinctions are consistent across the literature:
- Refractory disease: uricase therapy offers a meaningful response option when oral XOI therapy has failed or cannot be tolerated.
- Rapid urate lowering: the time to target is dramatically shorter with enzymatic degradation than with dose-titrated synthesis inhibition.
- Sustained control: XOIs can remain effective indefinitely in responsive patients, whereas uricase response may be limited by anti-drug antibody development.
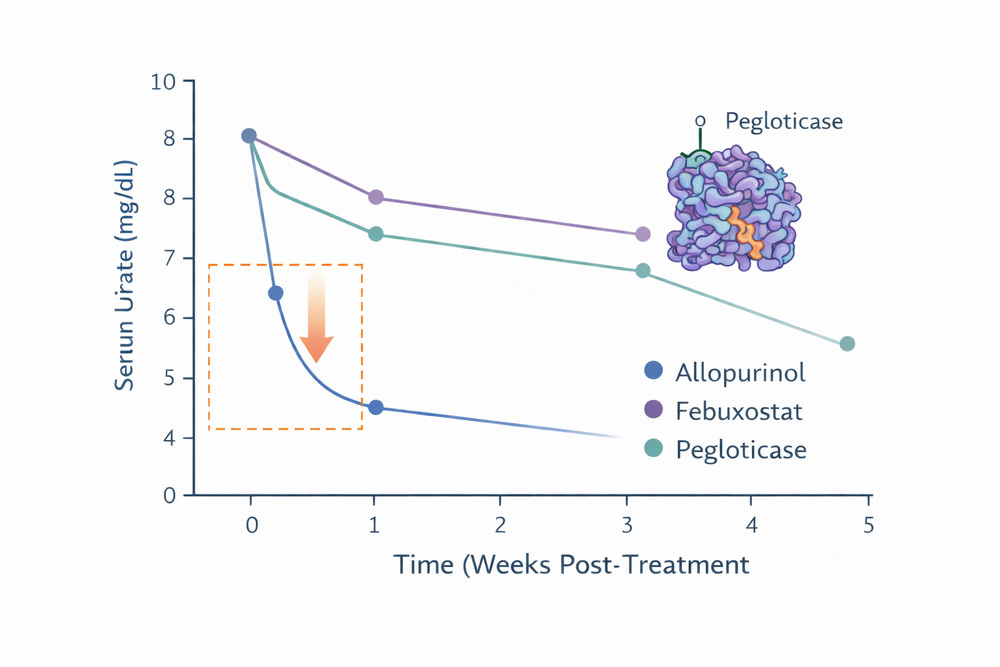
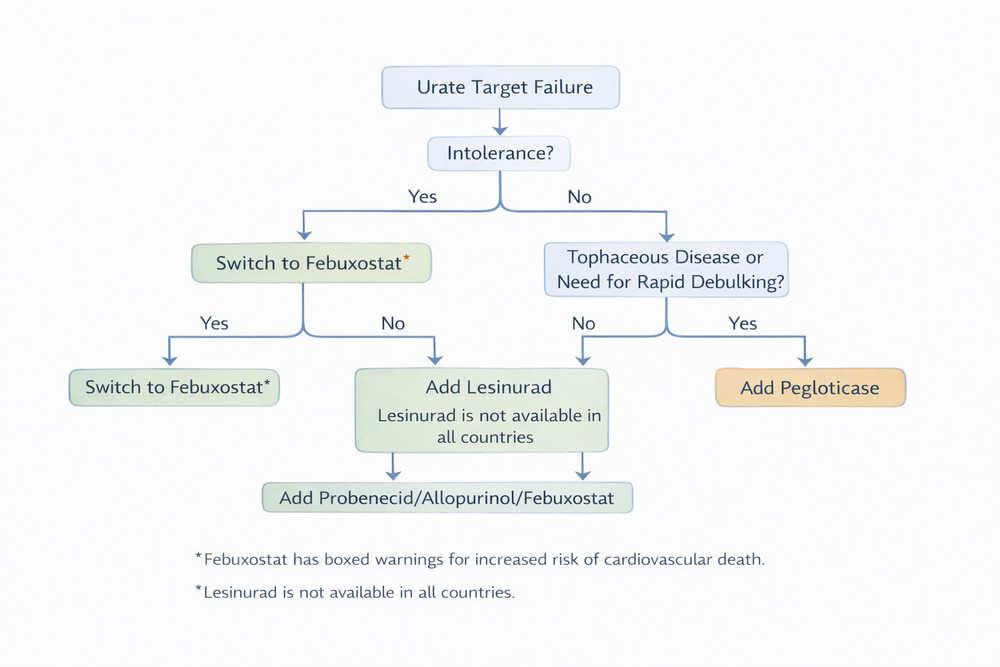
Fig 2–3. Suggested supporting visuals for efficacy kinetics and patient selection.
3.2 Safety Considerations
The safety profiles of these therapeutic classes reflect their distinct mechanisms and routes of administration. Oral XOIs are generally easier to manage longitudinally, but hypersensitivity and cardiovascular considerations remain important. Pegloticase introduces a different risk framework centered on infusion reactions, immunogenicity, flare burden during early treatment, and rare oxidative complications.
| Adverse Event | Allopurinol | Febuxostat | Pegloticase | Risk Mitigation |
|---|---|---|---|---|
| Severe cutaneous reactions | Rare but clinically serious | Rare | Not characteristic | Genetic screening where appropriate; early discontinuation if suspected |
| Cardiovascular concern | Generally neutral | Caution in high-risk populations | No equivalent boxed warning signal in the same framework | Risk-stratified prescribing and ongoing monitoring |
| Infusion reactions | Not applicable | Not applicable | Clinically important | Premedication, urate monitoring, and infusion protocols |
| Immunogenicity | Not a major limitation | Not a major limitation | Common cause of loss of response | Patient selection and immunomodulatory co-therapy strategies |
| Gout flares on initiation | Common | Common | Very common early in treatment | Prophylactic colchicine or NSAID support when appropriate |
Xanthine oxidase inhibitors are better suited for long-term foundational urate control in most patients, whereas uricase therapy is most compelling when rapid, deep urate reduction is needed or when standard oral therapy has clearly failed.
4. Clinical Relevance and Patient Selection
The choice between xanthine oxidase inhibition and uricase therapy should be driven by disease severity, prior treatment response, renal function, safety profile, and the practical urgency of urate lowering.
4.1 Situations Favoring XOI Therapy
- Newly diagnosed gout without major complications
- No history of failure or intolerance to oral urate-lowering therapy
- A preference for oral, daily self-administration
- Clinical scenarios where long-term maintenance is the primary goal
4.2 Situations Favoring Uricase Therapy
- Failure of maximally optimized or tolerated XOI therapy
- Documented intolerance to standard oral urate-lowering agents
- Severe tophaceous disease requiring rapid urate debulking
- Chronic kidney disease that complicates oral strategy selection
- Clinical need for faster urate reduction before procedural intervention
5. Research Implications
The mechanistic separation between synthesis inhibition and enzymatic degradation creates a useful framework for translational and pharmacologic research. Uricase-based interventions can produce rapid urate changes that are difficult to model with oral therapies alone, making them attractive for mechanistic studies of inflammation, renal biology, metabolism, and cardiovascular disease.
5.1 Combination and Sequencing Strategies
Combination or sequential treatment concepts remain scientifically attractive. In theory, uricase could be used for fast urate debulking, followed by xanthine oxidase inhibition for maintenance after the urate pool has been substantially reduced. Long-term implementation, however, remains constrained by immunogenicity and durability of response.
5.2 Biomarker and PK/PD Development
The relatively predictable exposure-response relationship of pegloticase supports pharmacokinetic and pharmacodynamic modeling, which may help refine dosing schedules, identify early non-response, and guide the broader development of therapeutic enzyme platforms.
For exploratory research, uricase offers a sharper experimental tool for manipulating serum urate, while XOIs remain more representative of real-world long-term maintenance therapy.
References
- Khanna, D., Fitzgerald, J. D., Khanna, P. P., et al. 2012 American College of Rheumatology guidelines for management of gout. Part 1: Systematic nonpharmacologic and pharmacologic therapeutic approaches to hyperuricemia. Arthritis Care & Research. 2012;64(10):1431-1446.
- Becker, M. A., Schumacher, H. R., Wortmann, R. L., et al. Pegloticase in patients with treatment-failure gout. New England Journal of Medicine. 2011;364(11):993-1004.
- Stamp, L. K., Day, R. O., and Yun, J. Allopurinol hypersensitivity: Investigating the cause and minimizing the risk. Nature Reviews Rheumatology. 2016;12(4):235-242.
- White, W. B., Saag, K. G., Becker, M. A., et al. Cardiovascular safety of febuxostat or allopurinol in patients with gout. New England Journal of Medicine. 2018;378(13):1200-1210.
- Sundy, J. S., Baraf, H. S. B., Yood, R. A., et al. Efficacy and tolerability of pegloticase for the treatment of chronic gout in patients refractory to conventional treatment. JAMA. 2011;306(7):711-720.