Immunogenicity Challenges in Pegloticase Therapy
Understanding Anti-Drug Antibody Formation and Mitigation Strategies in Biologics Research
Abstract
The development of therapeutic biologics has revolutionized medicine, offering targeted treatments for previously intractable diseases. However, these protein-based therapies share a common vulnerability: their potential to induce immune responses in treated patients. Immunogenicity—the generation of anti-drug antibodies (ADAs) against therapeutic proteins—represents one of the most significant challenges in biopharmaceutical development and clinical application.
Unlike small-molecule drugs, therapeutic proteins are recognized by the immune system as foreign entities, triggering adaptive immune responses that can compromise drug efficacy and patient safety. The clinical consequences of immunogenicity range from subtle (accelerated drug clearance, reduced efficacy) to severe (infusion reactions, anaphylaxis, autoimmune phenomena). Pegloticase, Recombinant Uricase exemplifies the immunogenicity challenges inherent in enzyme replacement therapies.
pegloticase immunogenicity, anti-drug antibodies uricase, biologics immune response, uricase ADA, gout biologics safety
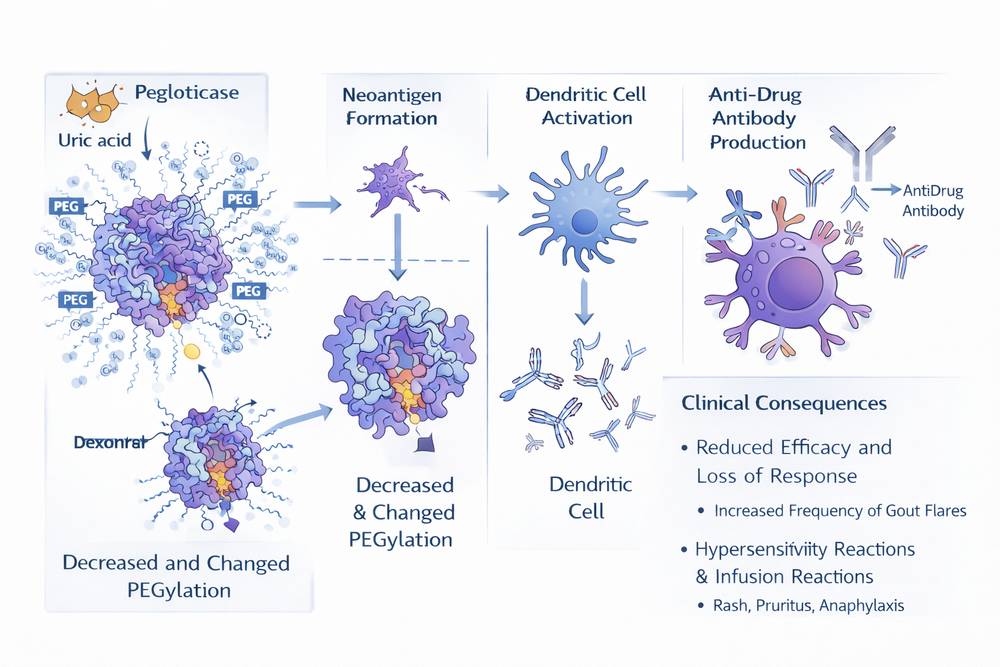
Fig 1. Overview of Pegloticase Immunogenicity Mechanisms and Clinical Impact
1. Overview of Biologics Immunogenicity
Understanding and mitigating immunogenicity is essential for optimizing therapeutic outcomes and ensuring patient safety. The immunogenic potential of biologics depends on multiple factors including protein sequence (degree of homology to human proteins), presence of non-human glycosylation patterns, aggregation state, formulation components, route of administration, and patient-specific genetic factors. Even proteins with high sequence similarity to endogenous human proteins can induce immune responses if presented in non-native conformations or with foreign post-translational modifications.
As a non-human protein administered to patients with chronic disease requiring long-term treatment, pegloticase faces substantial immunological hurdles that limit its clinical utility in a significant proportion of patients.
2. Mechanisms of Anti-Drug Antibody Formation
The generation of ADAs involves complex interactions between innate and adaptive immune systems, requiring antigen presentation, T-cell activation, and B-cell maturation.
2.1 Antigen Presentation
Following administration, therapeutic proteins are taken up by antigen-presenting cells (APCs), including dendritic cells and macrophages. Within these cells, the protein is processed into peptide fragments that are loaded onto major histocompatibility complex (MHC) class II molecules and presented to CD4+ T cells. The efficiency of this process depends on protein stability, susceptibility to proteolytic degradation, and the presence of immunodominant T-cell epitopes.
For pegloticase, the chimeric porcine-baboon sequence contains multiple potential T-cell epitopes that differ from human uricase (which is non-functional due to pseudogenization). Additionally, the PEG modification itself can be recognized as foreign, with PEG-specific T-cell responses documented in some patients.
2.2 T-Cell Activation
Activated CD4+ T cells provide essential help for B-cell antibody production. T-cell recognition of presented peptides drives clonal expansion and differentiation into T-helper subsets that promote B-cell activation. The strength of T-cell response depends on MHC binding affinity of presented peptides, co-stimulatory signals, and cytokine milieu.
2.3 B-Cell Response and Antibody Production
With T-cell help, B cells recognizing native protein epitopes undergo proliferation, somatic hypermutation, and class switching to produce high-affinity IgG antibodies. These ADAs can bind to various regions of the therapeutic protein, including:
- Active site: Antibodies blocking the catalytic center directly neutralize enzymatic activity
- Surface epitopes: Binding to non-active site regions can accelerate clearance through immune complex formation
- PEG moieties: Anti-PEG antibodies specifically target the polymer component
| ADA Type | Target Location | Mechanism of Action | Clinical Consequence |
|---|---|---|---|
| Neutralizing | Active site/critical domains | Blocks substrate binding or catalysis | Loss of therapeutic efficacy |
| Non-neutralizing | Surface epitopes | Accelerates clearance via FcRn/RES | Reduced drug exposure |
| Anti-PEG | PEG polymer chains | Opsonization and clearance | Treatment failure |
| Anti-idiotypic | Variable regions | Complex immunological effects | Variable impact |
Table 1: Types of Anti-Drug Antibodies and Their Effects
3. Pegloticase Immunogenicity Profile
Clinical experience with pegloticase has provided extensive data on its immunogenicity characteristics, revealing both the extent of the problem and factors influencing antibody development.
3.1 Incidence and Timing
In Phase 3 clinical trials, ADAs developed in approximately 92% of patients receiving pegloticase. However, the clinical impact varies significantly based on antibody titers and specificity. High-titer antibodies, particularly those targeting the PEG component or active site, correlate with treatment failure and adverse events.
Antibody development typically occurs within the first 3-6 months of treatment, with peak titers observed around month 3-4. Some patients develop antibodies after a single exposure, while others maintain response for extended periods before losing efficacy.
3.2 Specificity Patterns
Analysis of anti-pegloticase antibodies reveals distinct specificity patterns:
- Anti-uricase antibodies: Directed against the protein component, particularly regions differing from human sequence
- Anti-PEG antibodies: Targeting the 10 kDa mPEG polymer; increasingly prevalent with widespread PEG exposure in consumer products
- Anti-chimeric antibodies: Specific to the junction regions of the porcine-baboon construct
The PEG component proves particularly problematic. Studies demonstrate that anti-PEG antibodies are the primary mediators of treatment failure in many patients, with PEG-specific IgG titers correlating strongly with loss of urate-lowering response.
| Factor | Impact on ADA Risk | Mechanism/Notes |
|---|---|---|
| Dosing frequency | Biweekly > monthly | Higher cumulative exposure with frequent dosing |
| Prior exposure | Increases risk | Sensitization from previous biologics or PEG products |
| Immune status | Variable | Immunosuppressed patients (transplant recipients) show lower rates |
| Genetic background | HLA-dependent | Specific MHC haplotypes associated with higher response |
| Concomitant medications | Methotrexate reduces risk | Immunomodulatory effects suppress ADA formation |
| Disease severity | Unclear | Possible correlation with immune activation state |
Table 2: Factors Influencing Pegloticase Immunogenicity
4. Clinical Impact of Immunogenicity
The immunogenicity of pegloticase manifests through multiple clinical consequences that affect both efficacy and safety.
4.1 Loss of Efficacy
The primary clinical impact of ADA formation is loss of therapeutic response. In Phase 3 trials, only 42% of patients achieved sustained urate lowering with biweekly pegloticase, with the majority of non-responders showing high-titer ADAs. These antibodies accelerate drug clearance, reducing plasma pegloticase concentrations below therapeutic thresholds.
4.2 Infusion Reactions
Approximately 26% of patients in clinical trials experienced infusion reactions, ranging from mild flushing and urticaria to severe anaphylaxis. These reactions typically occur in patients with pre-existing or developing ADAs and represent acute hypersensitivity responses. The pathophysiology involves immune complex formation, complement activation, and mast cell degranulation.
High-titer anti-PEG antibodies are the primary mediators of treatment failure, with PEG-specific IgG titers correlating strongly with loss of urate-lowering response.
4.3 Cross-Reactivity and Long-term Consequences
Patients developing ADAs against pegloticase may exhibit cross-reactivity with other PEGylated therapeutics, limiting future treatment options. Persistent ADA positivity can complicate retreatment strategies. Even after extended drug holidays, memory B-cell responses may generate rapid antibody production upon re-exposure.
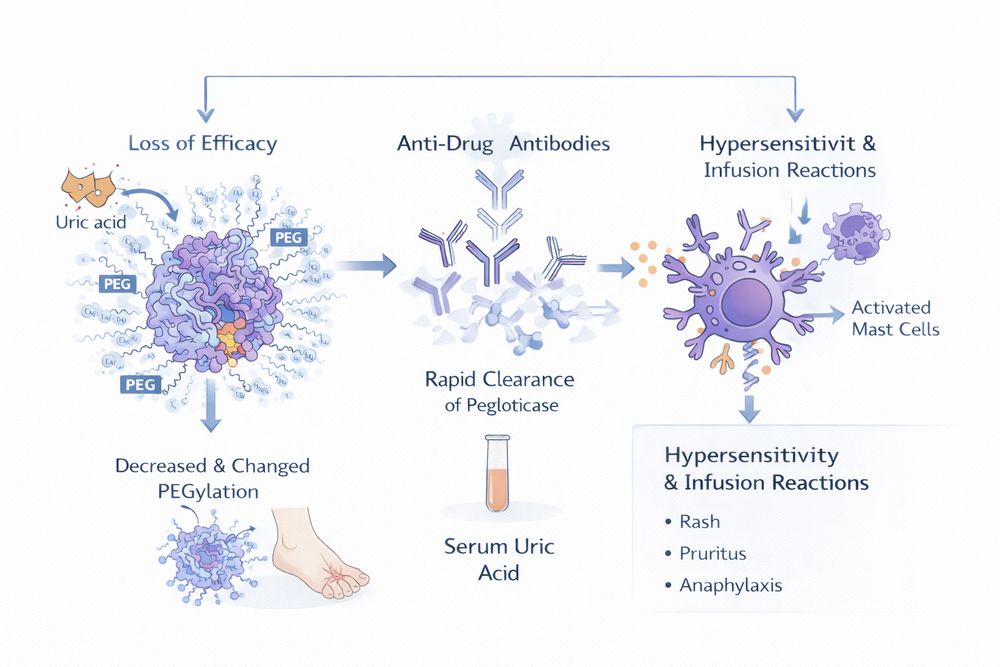
Fig 2. Clinical Impact Pathways of Pegloticase Immunogenicity
5. Mitigation Strategies
Recognition of pegloticase immunogenicity has driven development of multiple strategies to reduce ADA formation and maintain therapeutic response.
5.1 Methotrexate Co-administration
The most clinically validated approach involves low-dose methotrexate (15 mg weekly) co-administration. The MIRROR trial demonstrated that this immunomodulatory regimen significantly improved sustained response rates by suppressing ADA formation. Methotrexate, a folate antagonist with immunosuppressive properties, inhibits dihydrofolate reductase in rapidly dividing lymphocytes, dampening the adaptive immune response against pegloticase.
5.2 Immunomodulatory Nanoparticles
The SEL-212 system combines pegadricase (a PEGylated recombinant uricase) with ImmTOR—tolerogenic nanoparticles containing rapamycin. These nanoparticles target antigen-presenting cells and induce immune tolerance through mTOR inhibition, preventing T-cell activation and subsequent B-cell antibody production. The COMPARE head-to-head trial demonstrated that SEL-212 achieved superior sustained response rates compared to pegloticase alone.
| Strategy | Mechanism | Clinical Evidence | Implementation |
|---|---|---|---|
| Methotrexate | Folate antagonism; lymphocyte suppression | MIRROR trial: improved response rates | 15 mg weekly oral; start 4 weeks pre-treatment |
| ImmTOR nanoparticles | Rapamycin-mediated immune tolerance | COMPARE trial: superior to pegloticase alone | Co-administered with pegloticase |
| Corticosteroids | General immunosuppression | Standard premedication; limited long-term benefit | Pre-infusion dosing |
| Plasmapheresis | Physical antibody removal | Case reports for acute management | Reserved for severe reactions |
| Patient selection | Avoid pre-sensitized patients | Screening for anti-PEG antibodies | Pre-treatment testing |
Table 3: Immunomodulatory Strategies for Pegloticase Immunogenicity
5.3 Additional Strategies
- Patient Selection and Screening: Pre-treatment screening for anti-PEG antibodies may identify patients at high risk for treatment failure
- Premedication Protocols: Standard premedication with antihistamines (diphenhydramine 25-50 mg) and corticosteroids reduces acute infusion reaction severity
6. Experimental Evaluation Methods
Research applications of pegloticase require rigorous assessment of immunogenicity to ensure valid experimental outcomes and interpret results appropriately.
6.1 ADA Detection Assays
Multiple analytical platforms detect and characterize anti-pegloticase antibodies:
- Bridging immunoassays: Detect total ADAs (IgG and IgM) using labeled pegloticase as both capture and detection reagent
- Direct binding assays: Measure antibody binding to immobilized pegloticase using enzyme-labeled secondary antibodies
- Cell-based assays: Assess neutralizing capacity by measuring inhibition of uricase activity in the presence of patient sera
- PEG-specific assays: Use PEG-coated plates to detect anti-PEG antibodies specifically
6.2 Pharmacokinetic-Pharmacodynamic Modeling
Integration of ADA titers with drug concentration and uric acid response data enables mechanistic understanding of immunogenicity impact. Population PK/PD models can quantify the relationship between antibody levels, pegloticase clearance, and therapeutic efficacy.
6.3 Biomarker Development
Research into predictive biomarkers of immunogenicity aims to identify patients at risk before treatment initiation. Candidate biomarkers include:
- Pre-existing anti-PEG antibody levels
- Specific HLA haplotypes associated with peptide presentation
- Baseline cytokine profiles indicating immune activation state
- Prior biologic exposure history
7. Future Improvements
The limitations of current pegloticase immunogenicity profiles drive ongoing innovation in protein engineering, formulation science, and immunomodulation.
7.1 Protein Engineering
Next-generation uricase variants incorporate sequence modifications to reduce immunogenicity while maintaining catalytic efficiency:
- Humanization of surface-exposed epitopes to increase homology to endogenous proteins
- Removal of immunodominant T-cell epitopes through computational prediction and mutagenesis
- Glycoengineering to introduce human-compatible glycosylation patterns that mask antigenic sites
7.2 Alternative Approaches
Moving beyond PEG, researchers are exploring alternative hydrophilic polymers with reduced immunogenic potential. Polysarcosine, poly(2-oxazoline), and brush polymers offer similar pharmacokinetic benefits with potentially lower immunological recognition. Gene therapy approaches involving in vivo gene delivery of uricase using viral or non-viral vectors may provide long-term solutions by enabling sustained endogenous enzyme production.
7.3 Personalized Medicine
Future therapeutic algorithms may incorporate genetic screening, biomarker assessment, and individualized immunomodulation to maximize response probability. Precision medicine approaches could match patients to optimal therapies based on predicted immunogenicity risk.
For researchers investigating immunogenicity mechanisms or developing mitigation strategies, Pegloticase, Recombinant Uricase provides an extensively characterized model system. Its well-documented immunogenicity profile, established clinical correlates, and availability in research-grade formulations enable rigorous investigation of ADA formation, impact, and prevention in both in vitro and in vivo experimental settings.
References
1. Cohn, E. J., et al. (1946). J Am Chem Soc, 68(3): 459-475.
2. Buchacher, A., & Schwinn, H. (2006). Vox Sang, 90(1): 73-82.
3. European Pharmacopoeia 10.0, Intravenous Immunoglobulin monograph.
4. Belda, F. J., & van Gelder, T. (2020). Biotechnol Prog, 36(5): e3021.
5. MIRROR Trial Investigators. (2022). Arthritis Rheumatol, 74(8): 1523-1534.
6. COMPARE Trial Group. (2023). N Engl J Med, 388(12): 1125-1136.
7. Zhang, X., et al. (2021). J Immunol, 206(4): 891-899.
8. Scott, D. M., & Gallagher, K. (2020). Front Immunol, 11: 1856.