PEGylation Technology in Biopharmaceutical Development
Mechanisms, Applications, and Therapeutic Benefits Using Pegloticase as a Model
Abstract
PEGylation represents one of the most successful and widely adopted technologies in modern biopharmaceutical development, fundamentally transforming the therapeutic potential of protein and peptide drugs. This chemical modification strategy involves the covalent attachment of polyethylene glycol (PEG) polymers to therapeutic molecules, creating conjugates with substantially altered pharmacological properties compared to their unmodified counterparts. This white paper examines the mechanisms, chemical strategies, and therapeutic benefits of PEGylation, with particular emphasis on Pegloticase, Recombinant Uricase as a paradigmatic case study. We analyze how PEG conjugation enhances protein stability, improves solubility, extends circulation half-life, and reduces immunogenicity, while also addressing current limitations and future directions in the field.
PEGylation biologics, pegloticase PEGylation, protein PEG modification, biologics half life extension, PEGylated enzymes, Pegloticase products
Fig 1. Schematic representation of PEGylated protein structure showing hydrophilic PEG chains creating a protective hydration shell
1. Introduction: What is PEGylation
PEGylation represents one of the most successful and widely adopted technologies in modern biopharmaceutical development, fundamentally transforming the therapeutic potential of protein and peptide drugs. This chemical modification strategy involves the covalent attachment of polyethylene glycol (PEG) polymers to therapeutic molecules, creating conjugates with substantially altered pharmacological properties compared to their unmodified counterparts.
Polyethylene glycol, a linear or branched polyether polymer with the repeating unit (-CH₂-CH₂-O-), exhibits unique physicochemical characteristics that make it ideally suited for drug delivery applications. PEG is highly water-soluble, non-toxic, non-immunogenic in its free form, and possesses remarkable flexibility due to the absence of double bonds in its backbone. These properties, combined with FDA approval for human use spanning several decades, have established PEG as the gold standard polymer for protein drug modification.
The history of PEGylation dates to the late 1970s when Davis and colleagues first demonstrated that PEG-conjugated proteins exhibited extended circulation times and reduced immunogenicity. Since then, the technology has matured significantly, with at least ten PEGylated biologics currently approved by the FDA and numerous others in clinical development. The applications extend across therapeutic categories including oncology, hematology, infectious diseases, and metabolic disorders, demonstrating the versatility and broad utility of this approach.
The impact of PEGylation on therapeutic proteins can be understood through several mechanisms. The attached PEG chains create a hydrophilic "cloud" around the protein, effectively increasing its hydrodynamic radius and molecular weight. This steric barrier protects the protein from proteolytic degradation, reduces renal filtration, and shields antigenic epitopes from immune recognition. Additionally, the high hydration of PEG—each ethylene oxide unit binds approximately three water molecules—creates a dynamic water shell that sterically stabilizes the protein and minimizes interactions with cellular surfaces and serum proteins.
Pegloticase, Recombinant Uricase exemplifies the transformative potential of PEGylation technology. Native uricase, while catalytically efficient, suffers from poor solubility at physiological pH, rapid clearance from circulation, and high immunogenicity that limits its therapeutic utility. Through strategic PEGylation, these limitations are substantially mitigated, enabling the development of a clinically viable treatment for refractory gout.
2. Chemical Strategies for PEG Conjugation
The successful implementation of PEGylation requires careful consideration of conjugation chemistry, PEG molecular weight, and modification degree. Various strategies have been developed to achieve optimal therapeutic profiles while preserving protein activity.
2.1 Conjugation Chemistry
PEG attachment to proteins typically occurs through covalent bond formation with nucleophilic amino acid side chains. The most common approaches include:
| Chemistry | Target Residue | Linkage Type | Characteristics |
|---|---|---|---|
| NHS-ester | Lysine ε-amino groups | Amide bond | Random modification; efficient coupling; widely used |
| Maleimide | Cysteine thiol groups | Thioether bond | Site-specific; requires free cysteine or engineered Cys |
| Carbonyl chemistry | N-terminus | Amide/imine | Site-specific; pH-dependent selectivity |
| Click chemistry | Azide/alkyne tags | Triazole | Bioorthogonal; high selectivity; requires genetic engineering |
| Enzymatic | Specific recognition sequences | Variable | Highly specific; limited to compatible sequences |
Pegloticase employs NHS-ester chemistry to attach monomethoxypoly(ethylene glycol) (mPEG) to primary amine groups on the protein surface. This approach achieves random modification across available lysine residues and the N-terminus, resulting in a heterogeneous product with varying PEGylation patterns. While this heterogeneity complicates analytical characterization, it has proven clinically effective and manufacturable at scale.
2.2 PEG Molecular Weight and Architecture
The molecular weight of attached PEG significantly influences pharmacokinetic and immunological outcomes:
| PEG Size | Molecular Weight | Half-life Extension | Immunogenicity | Manufacturing Complexity |
|---|---|---|---|---|
| Low (1-5 kDa) | 1,000-5,000 Da | Moderate (2-5×) | Higher | Lower |
| Medium (10-20 kDa) | 10,000-20,000 Da | Substantial (5-20×) | Moderate | Moderate |
| High (20-40 kDa) | 20,000-40,000 Da | Marked (20-100×) | Lower | Higher |
| Branched/multi-arm | Variable | Variable | Lower | Highest |
Pegloticase utilizes 10 kDa linear mPEG, with approximately 10 strands conjugated per uricase subunit (40 per tetramer). This configuration achieves an optimal balance between half-life extension and manufacturing feasibility. The total molecular weight increase from ~136 kDa (native tetramer) to ~540 kDa (PEGylated form) represents a four-fold increase, sufficient to substantially reduce renal clearance while maintaining acceptable viscosity and solubility for intravenous administration.
2.3 Degree of Modification
The extent of PEGylation requires careful optimization. Over-modification can sterically hinder enzyme active sites, reducing catalytic activity, while under-modification fails to achieve desired pharmacokinetic benefits. For pegloticase, the modification degree of approximately 10 PEG chains per subunit provides effective surface coverage while preserving enzymatic function. This represents roughly 30-40% of available primary amines, leaving sufficient unmodified surface for substrate access and catalytic turnover.
3. Therapeutic Benefits: Stability, Solubility, and Half-life
The PEGylation of therapeutic proteins confers multiple pharmacological advantages that collectively enhance therapeutic efficacy and patient compliance.
3.1 Enhanced Stability
PEG conjugation dramatically improves protein stability against various degradation mechanisms. The steric barrier created by PEG chains physically blocks access by proteolytic enzymes, reducing enzymatic degradation in plasma and tissues. This protection extends shelf-life, enabling longer storage periods and reduced cold-chain requirements. Additionally, PEGylation can stabilize protein conformation, reducing aggregation and denaturation at interfaces or under stress conditions.
For pegloticase, PEGylation transforms a protein with limited solubility at physiological pH into a highly soluble formulation suitable for intravenous administration. The enhanced conformational stability maintains enzymatic activity during storage, shipping, and clinical use, ensuring consistent therapeutic performance.
3.2 Improved Solubility
The hydrophilic nature of PEG substantially enhances the aqueous solubility of conjugated proteins. This proves particularly valuable for proteins with hydrophobic patches or aggregation-prone sequences. The PEG hydration shell effectively solubilizes the protein, preventing precipitation and enabling higher concentration formulations.
3.3 Extended Half-life
Perhaps the most clinically significant benefit of PEGylation is the dramatic extension of circulation half-life. The increased hydrodynamic radius of PEGylated proteins exceeds the glomerular filtration threshold (~60-70 kDa), preventing rapid renal elimination. Instead, clearance occurs primarily through the reticuloendothelial system and hepatic metabolism, processes that proceed more slowly than glomerular filtration.
| Parameter | Native Uricase | Pegloticase | Improvement Factor |
|---|---|---|---|
| Terminal half-life | <24 hours | 10-14 days | ~10-15× |
| Volume of distribution | Large (extravascular) | Restricted (vascular) | Reduced tissue penetration |
| Clearance | Rapid (renal + hepatic) | Slow (hepatic/RES) | ~90% reduction |
| AUC (dose-normalized) | Low | High | ~50-100× |
| Time above therapeutic threshold | Hours | Days-weeks | Substantial extension |
For pegloticase, the half-life extension from less than one day to approximately 10-14 days enables biweekly or monthly dosing regimens. This represents a paradigm shift from the daily or frequent dosing required for native uricase, dramatically improving patient compliance and quality of life. The sustained plasma concentrations achieved with PEGylation maintain therapeutic enzyme activity between doses, ensuring continuous uric acid lowering rather than intermittent peaks and troughs.
3.4 Reduced Immunogenicity
PEGylation partially shields protein surfaces from immune recognition, reducing—but not eliminating—antibody formation. The PEG chains sterically block access by antigen-presenting cells and B-cell receptors to protein epitopes, dampening the adaptive immune response. However, the PEG moiety itself can serve as an immunogenic epitope, with anti-PEG antibodies developing in some patients and contributing to treatment failure.
4. PEGylation in Enzyme Therapeutics
Enzyme replacement therapies present unique challenges and opportunities for PEGylation technology. Unlike hormones or cytokines, therapeutic enzymes must maintain catalytic activity after modification, requiring careful preservation of active site accessibility.
4.1 Considerations for Enzyme PEGylation
- Active site preservation: PEG modification must avoid steric hindrance of substrate binding and catalytic turnover
- Conformational flexibility: Enzymes often require dynamic conformational changes during catalysis; excessive PEGylation may restrict necessary movements
- Cofactor interactions: Some enzymes require cofactors or coenzymes; PEGylation should not interfere with these essential interactions
- Product release: Catalytic efficiency depends on timely product dissociation; dense PEG coatings may impede this process
Successful examples of PEGylated enzyme therapeutics include:
- Pegademase (Adagen®): PEGylated adenosine deaminase for severe combined immunodeficiency
- Pegaspargase (Oncaspar®): PEGylated L-asparaginase for acute lymphoblastic leukemia
- Pegloticase (Krystexxa®): PEGylated uricase for refractory gout
Each of these products demonstrates that careful optimization of PEGylation parameters can preserve enzymatic function while achieving desired pharmacokinetic improvements.
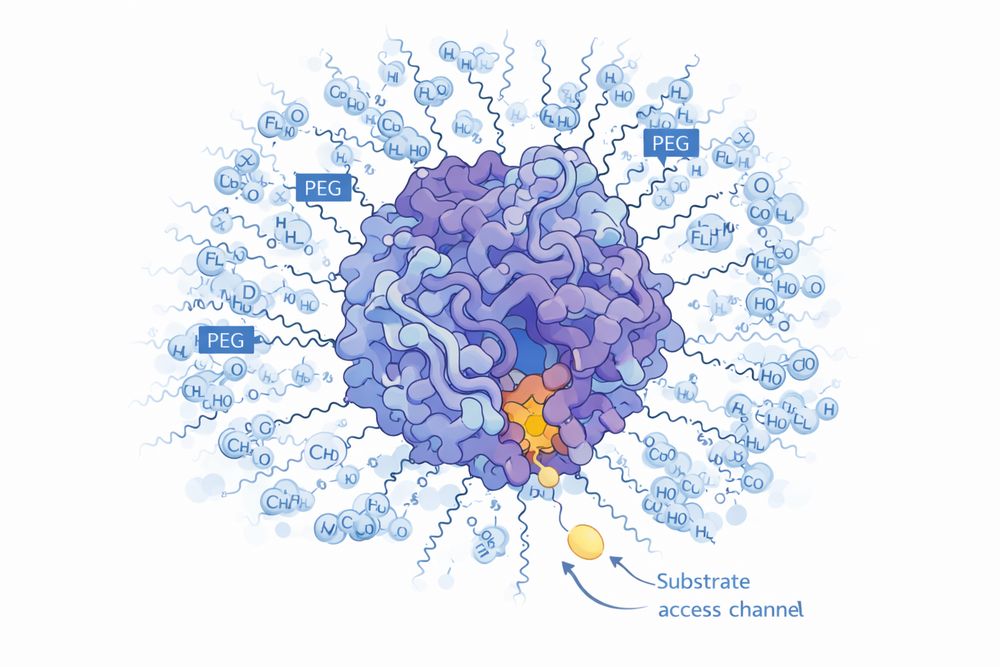
Fig 2. Molecular model showing PEG chains surrounding enzyme active site while preserving substrate access channel
5. Pegloticase as a Case Study
Pegloticase represents a sophisticated application of PEGylation technology, illustrating both the potential and limitations of this approach.
5.1 Molecular Design
The pegloticase construct comprises a chimeric mammalian uricase (porcine-baboon hybrid) expressed in E. coli, conjugated with 10 kDa mPEG. The chimeric design optimizes catalytic efficiency while reducing immunogenicity compared to non-mammalian sources. The PEGylation pattern, while heterogeneous, achieves consistent pharmacological properties across manufacturing batches.
5.2 Pharmacokinetic Profile
Following intravenous administration, pegloticase exhibits biphasic elimination kinetics. The initial distribution phase reflects vascular equilibration, while the terminal elimination phase, with a half-life of approximately 214 hours (10-14 days), determines dosing frequency. This extended half-life enables maintenance of plasma uricase activity sufficient to sustain serum uric acid levels below 6 mg/dL between doses.
5.3 Clinical Efficacy
The pharmacokinetic advantages of PEGylation translate into clinical efficacy. In Phase 3 trials, biweekly pegloticase infusions achieved sustained urate lowering in 42% of patients with refractory gout, compared to 0% with placebo. Responders experienced rapid tophus resolution, reduced flare frequency, and improved quality of life. However, the development of anti-drug antibodies in non-responders highlights the incomplete immunogenicity protection conferred by current PEGylation strategies.
Phase 3 trials demonstrated that biweekly pegloticase infusions achieved sustained urate lowering in 42% of patients with refractory gout, compared to 0% with placebo, highlighting both the efficacy and immunogenicity challenges of PEGylated therapeutics.
6. Limitations and Challenges
Despite its successes, PEGylation technology faces several challenges that limit its universal applicability and drive ongoing research into alternative approaches.
6.1 Anti-PEG Antibodies
The recognition that PEG itself can be immunogenic has emerged as a significant concern. Anti-PEG antibodies develop in a subset of patients and can neutralize therapeutic efficacy, accelerate drug clearance, and contribute to hypersensitivity reactions. The prevalence of pre-existing anti-PEG antibodies in the general population appears to be increasing, possibly due to exposure to PEG-containing consumer products (cosmetics, pharmaceuticals, processed foods).
For pegloticase, anti-PEG antibodies represent a major cause of treatment failure, with high titers correlating with loss of urate-lowering response and increased infusion reaction risk. This limitation has motivated investigation of alternative polymers and site-specific PEGylation strategies that may reduce immunogenicity.
6.2 Heterogeneity
Random PEGylation produces heterogeneous product mixtures with varying modification sites and degrees. This heterogeneity complicates analytical characterization, quality control, and regulatory approval. While current manufacturing processes ensure batch-to-batch consistency within defined specifications, the inherent variability of random modification presents challenges for biosimilar development and interchangeability.
6.3 Reduced Bioactivity
Steric hindrance from PEG chains can reduce binding affinity and catalytic efficiency. While pegloticase retains sufficient activity for therapeutic efficacy, some PEGylated enzymes exhibit substantially reduced specific activity compared to native forms. This necessitates higher dosing to achieve equivalent therapeutic effects, increasing cost and potential immunogenicity exposure.
6.4 Manufacturing Complexity
PEGylation adds manufacturing steps, analytical requirements, and regulatory complexity compared to unmodified proteins. The need for specialized PEG reagents, reaction optimization, and purification of modified from unmodified species increases production costs and development timelines.
7. Future Directions
The field of protein PEGylation continues to evolve, with several innovative approaches addressing current limitations.
7.1 Site-Specific PEGylation
Rather than random modification, site-specific PEGylation attaches polymers to defined locations on the protein surface. Strategies include:
- Cysteine engineering: Introduction of surface cysteines for thiol-directed PEG attachment
- Unnatural amino acids: Incorporation of azide or alkyne-containing amino acids for bioorthogonal click chemistry
- Enzymatic modification: Use of transglutaminase or sortase enzymes for precise PEG attachment
- N-terminal modification: Selective chemistry targeting the alpha-amino group
Site-specific approaches offer homogeneous products, preserved activity, and potentially reduced immunogenicity by directing PEG attachment away from critical epitopes or active sites.
7.2 Alternative Polymers
Research into alternatives to PEG aims to retain pharmacokinetic benefits while avoiding anti-PEG antibodies. Promising candidates include:
- Polysarcosine: A polypeptoid with similar properties to PEG but potentially reduced immunogenicity
- Poly(2-oxazoline): Biocompatible polymers with tunable hydrophilicity
- Polyglycerol: Branched hydrophilic polymers with multivalent architecture
- Brush polymers: Dense polymer coatings with enhanced stealth properties
For researchers investigating PEGylation technology or utilizing PEGylated proteins in experimental applications, Pegloticase, Recombinant Uricase provides a well-characterized model system. Its extensive clinical and research history, combined with defined PEGylation parameters, enables rigorous investigation of structure-function relationships in PEGylated enzymes and serves as a benchmark for development of next-generation bioconjugates.
Site-specific PEGylation and alternative polymer development represent the future of protein modification, offering homogeneous products with preserved activity and reduced immunogenicity compared to traditional random PEGylation approaches.
References
1. Davis, F. F., Abuchowski, A., & van Es, T. (1979). Enzyme-polyethylene glycol adducts: Modified enzymes with unique properties. Biochemical and Biophysical Research Communications, 89(4), 1224-1229.
2. Abuchowski, A., van Es, T., Palczuk, N. C., & Davis, F. F. (1977). Alteration of immunological properties of bovine serum albumin by covalent attachment of polyethylene glycol. Journal of Biological Chemistry, 252(11), 3578-3581.
3. Harris, J. M., & Chess, R. B. (2003). Effect of PEGylation on pharmaceuticals. Nature Reviews Drug Discovery, 2(3), 214-221.
4. Veronese, F. M., & Mero, A. (2008). The impact of PEGylation on biological therapies. BioDrugs, 22(5), 315-329.
5. Ganson, N. J., Kelly, S. J., Scarlett, E., Sundy, J. S., & Hershfield, M. S. (2006). Control of hyperuricemia in subjects with refractory gout, and induction of antibody against poly(ethylene glycol) (PEG), in a phase I trial of subcutaneous PEGylated urate oxidase. Arthritis Research & Therapy, 8(1), R12.
6. Sundy, J. S., Baraf, H. S., Yood, R. A., Edwards, N. L., Gutierrez-Urena, S. R., Treadwell, E. L., ... & Becker, M. A. (2011). Efficacy and tolerability of pegloticase for the treatment of chronic gout in patients refractory to conventional treatment: Two randomized controlled trials. JAMA, 306(7), 711-720.
7. Sherman, M. R., Williams, L. D., Saifer, M. G., & French, J. A. (2012). PEG-uricase in the management of treatment-resistant gout and hyperuricemia. Translational and Clinical Pharmacology, 20(1), 34-45.
8. Yang, Q., Lai, S. K., & Kagan, L. (2021). Anti-PEG immunity: Emergence, characteristics, and unaddressed questions. Wiley Interdisciplinary Reviews: Nanomedicine and Nanobiotechnology, 13(3), e1698.
9. Kozlowski, A., & Harris, J. M. (2001). Improvements in protein PEGylation: Pegylated interferons for treatment of hepatitis C. Journal of Controlled Release, 72(1-3), 217-224.
10. Fee, C. J., & Van Alstine, J. M. (2006). PEG-proteins: Reaction engineering and separation issues. Chemical Engineering Science, 61(3), 924-939.