Uricase Therapy Review
A Comparative Review of Pegloticase, Rasburicase, and Emerging Uricase-Based Therapies
Abstract
Uricase-based therapy has reshaped the treatment landscape for severe hyperuricemia and refractory gout by introducing an enzymatic route for urate elimination. Unlike xanthine oxidase inhibitors and uricosuric agents, uricase therapeutics directly convert uric acid into allantoin, a far more soluble metabolite that is readily cleared from the body.
This review summarizes the development of uricase therapeutics, compares rasburicase and pegloticase, outlines key clinical data, and discusses the major limitations of current therapy, especially immunogenicity and infusion-related safety concerns. It also highlights next-generation candidates and future strategies intended to improve durability, convenience, and response rates in advanced gout management.
uricase therapy review, pegloticase vs rasburicase, gout biologics development, uric acid-lowering therapies, recombinant uricase clinical review, Pegloticase, Recombinant Uricase
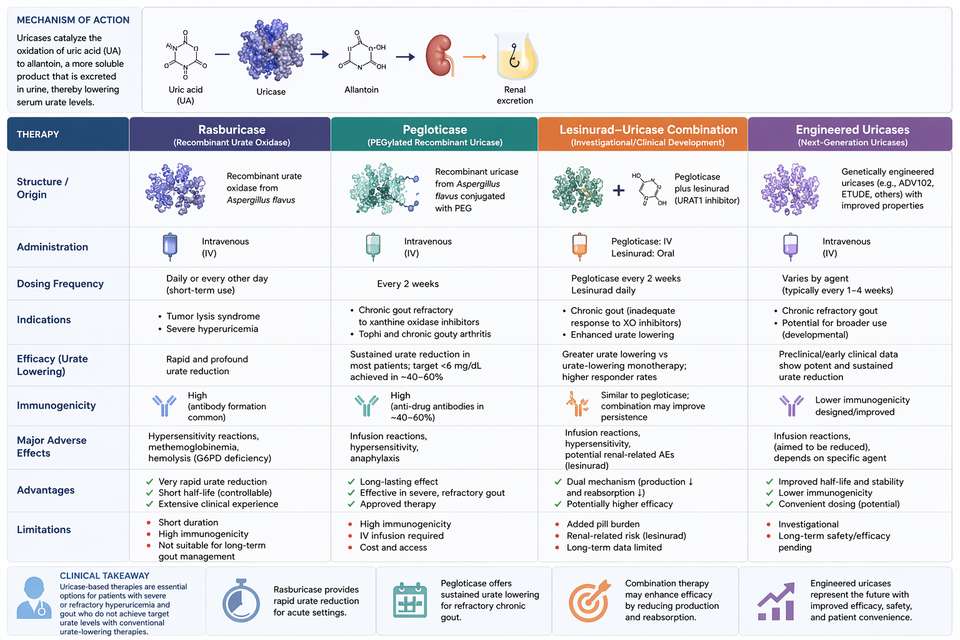
Fig 1. Comparative overview of uricase-based therapies for hyperuricemia and gout
1. Overview of Uric Acid-Lowering Strategies
Over the past two decades, gout management has evolved from symptomatic control toward targeted disease modification. Traditional therapies mainly rely on xanthine oxidase inhibition to reduce uric acid synthesis or on uricosuric drugs to enhance renal urate excretion. Although these approaches are effective in many patients, a meaningful subset continues to experience persistent hyperuricemia, recurrent flares, and progressive tophaceous disease despite optimized therapy.
Uricase-based therapies address this unmet need through a fundamentally different mechanism. Rather than modulating synthesis or excretion alone, they catalyze the oxidation of uric acid into allantoin, thereby introducing an extrarenal urate-lowering pathway. This makes uricase therapy particularly relevant in severe refractory gout and in patients with major limitations in conventional treatment response.
2. History of Uricase Therapeutics
The therapeutic utility of uricase was recognized long before recombinant protein engineering became feasible. Early work relied on fungal uricase, which showed strong catalytic activity but also high immunogenicity, short plasma persistence, and limited suitability for chronic disease use.
Recombinant technology enabled more consistent production and protein optimization. Rasburicase, a recombinant uricase derived from Aspergillus flavus, became an important option for tumor lysis syndrome because of its rapid onset of action. However, its lack of PEGylation and relatively short half-life limited its practicality in chronic gout.
Pegloticase was developed to address these limitations. By combining a chimeric mammalian uricase backbone with extensive PEGylation, it achieved longer circulation time and a dosing schedule appropriate for chronic refractory gout, marking a major step forward in biologic urate-lowering therapy.
3. Rasburicase vs Pegloticase: Comparative Analysis
3.1 Core Pharmacologic Differences
| Characteristic | Rasburicase | Pegloticase | Clinical Implication |
|---|---|---|---|
| Source organism | Aspergillus flavus (fungal) | Porcine-baboon chimera (mammalian) | Different immunogenicity profiles |
| Expression system | Saccharomyces cerevisiae | Escherichia coli | Different manufacturing strategies |
| PEGylation | None | 10 kDa mPEG (~40 strands per tetramer) | Extends half-life and reduces immune exposure |
| Molecular weight | ~136 kDa | ~540 kDa | Pegloticase exceeds the renal filtration threshold |
| Terminal half-life | ~18–24 hours | ~10–14 days | Pegloticase supports chronic intermittent dosing |
| FDA indication | Tumor lysis syndrome | Chronic refractory gout | Distinct clinical roles |
| Standard dosing | 0.15–0.2 mg/kg daily × 5 days | 8 mg IV every 2 weeks | Pegloticase is optimized for long-term disease management |
| Immunogenicity | High | Moderate but still clinically significant | Both require careful monitoring |
These molecular differences directly determine clinical utility. Rasburicase is well suited for short-term rapid urate reduction, especially in oncology settings. Pegloticase, in contrast, was engineered for repeated administration in adult patients with uncontrolled gout and remains the benchmark biologic in this disease space.
Rasburicase is ideal for acute, short-duration urate control, while Pegloticase, Recombinant Uricase is specifically designed for sustained management of chronic refractory gout.
4. Clinical Indications and Efficacy
4.1 Pegloticase in Refractory Gout
Pegloticase has shown its greatest value in the most difficult gout population: patients with chronic refractory disease who do not respond adequately to or cannot tolerate conventional urate-lowering therapy. In pivotal Phase 3 studies, biweekly intravenous pegloticase produced sustained serum urate control in a meaningful portion of patients and was associated with tophus reduction, fewer flares over time, and improved quality of life among responders.
4.2 Key Clinical Trials
| Study | Design | Population | Primary Endpoint | Key Findings |
|---|---|---|---|---|
| Phase 3 RCTs | Randomized, double-blind, placebo-controlled | 225 patients with refractory gout | Plasma uric acid <6 mg/dL at months 3 and 6 | 42% responders with biweekly dosing; rapid tophus improvement in responders |
| Open-label extension | Long-term follow-up | 149 prior completers | Safety and sustained response | Responders maintained urate control and showed reduced flare burden over time |
| Phase II transplant study | Open-label | 30 patients including transplant recipients | Urate normalization and safety | Durable response in a subset; lower immunogenicity in immunosuppressed settings |
| MIRROR trial | Pegloticase + methotrexate | Patients with uncontrolled gout | Improved sustained response | Methotrexate co-therapy enhanced durability by reducing anti-drug antibody formation |
These findings support pegloticase as a high-impact option for carefully selected patients, particularly when long-standing urate burden, tophi, and ongoing symptoms persist despite optimized standard care.
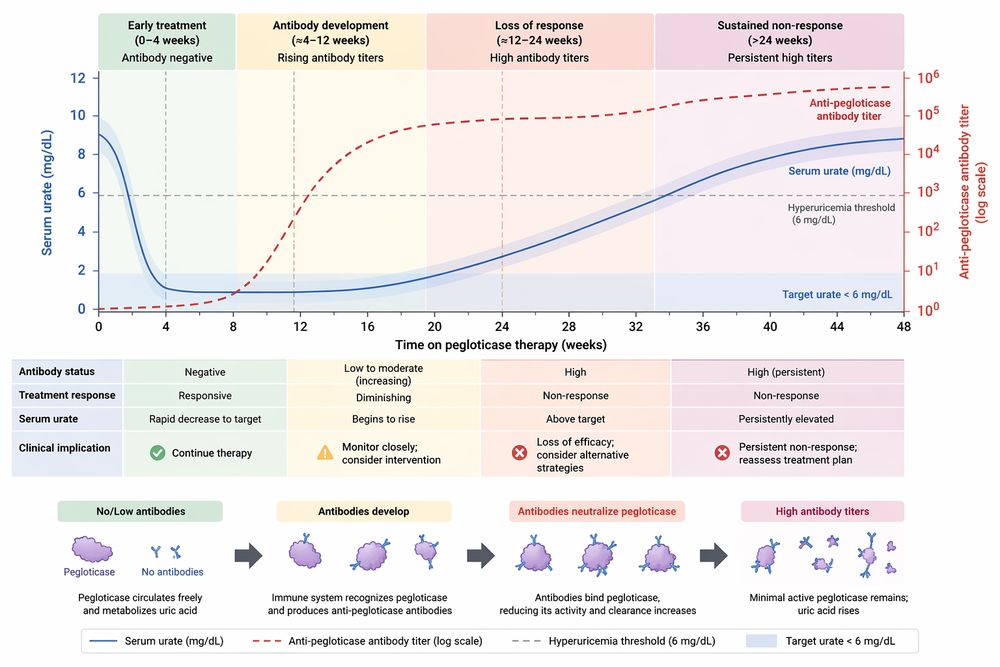
Fig 2. Relationship between anti-pegloticase antibody development and treatment response over time
5. Safety Concerns and Anti-Drug Antibody Issues
The major limitations of current uricase therapy are immunogenicity and infusion-related adverse events. Pegloticase can cause infusion reactions ranging from mild cutaneous symptoms to severe hypersensitivity and anaphylaxis. Because of this, treatment is typically delivered in controlled clinical settings with premedication and close observation.
Gout flares also commonly occur during early treatment because rapid urate reduction mobilizes existing monosodium urate crystal deposits. Although counterintuitive, this flare pattern reflects active urate depletion and usually improves with ongoing response and flare prophylaxis.
5.1 Anti-Drug Antibodies
Anti-drug antibodies remain the central barrier to durable benefit. They can accelerate drug clearance, reduce serum exposure, neutralize activity, and increase the risk of infusion reactions. Antibodies may target both the uricase protein and the PEG component, which explains why some patients lose response despite initial urate lowering.
5.2 Strategies to Reduce Immunogenicity
- Methotrexate co-administration: now a major response-enhancing strategy in clinical practice and trials.
- Immunomodulatory nanoparticle platforms: designed to induce tolerance and reduce adaptive immune activation.
- Patient selection: exclusion of high-risk immune profiles may improve safety and treatment persistence.
- Dosing optimization: biweekly treatment has generally produced better durability than less frequent schedules.
Immunogenicity is the main reason pegloticase loses efficacy over time. Current and next-generation development programs increasingly focus on preventing or delaying antibody formation rather than changing catalytic potency alone.
6. Emerging Next-Generation Uricase Drugs
Current limitations have driven the development of more advanced uricase-based platforms. These programs aim to preserve the rapid urate-lowering power of enzymatic therapy while improving durability, reducing immune recognition, and simplifying treatment logistics.
6.1 Leading Development Directions
- SEL-212 (Pegadricase + ImmTOR): combines a PEGylated uricase with tolerogenic nanoparticles intended to suppress anti-drug antibody formation.
- Engineered uricases: sequence redesign, site-specific PEGylation, and alternative polymer conjugates are being explored to reduce immunogenicity.
- Competitive non-uricase approaches: novel urate transporter inhibitors may challenge biologics in some refractory populations.
- Gene therapy concepts: long-term uricase expression remains an attractive but still early-stage strategy.
7. Future Perspectives
The future of uricase therapy will likely be shaped by precision immunogenicity management, smarter combination regimens, and more convenient delivery systems. Companion diagnostics could identify patients most likely to form anti-drug antibodies, while tailored immunomodulation may help sustain response without excessive safety tradeoffs.
Subcutaneous delivery, longer-acting formulations, and personalized treatment algorithms may further expand the therapeutic utility of biologic urate lowering. Even as new candidates emerge, Pegloticase, Recombinant Uricase remains the benchmark against which future uricase platforms are measured.
8. Conclusion
Uricase therapy has established a distinct and clinically important role in severe hyperuricemia by introducing direct enzymatic urate degradation. Rasburicase and pegloticase represent two different therapeutic models: one optimized for rapid short-term control and the other designed for repeated administration in chronic refractory gout.
Despite major advances, the field is still constrained by immune-mediated loss of response and infusion-related safety concerns. Continued innovation in immune tolerance, protein engineering, and delivery technology is likely to define the next era of uricase therapeutics.
For refractory gout research and advanced therapeutic evaluation, pegloticase remains the most established uricase platform, while next-generation candidates are being developed to improve durability, safety, and long-term patient benefit.
References
1. Clinical and translational literature on uricase-based therapy for hyperuricemia and gout.
2. Pharmacology and development history of rasburicase and pegloticase.
3. Phase 3 and extension studies evaluating pegloticase efficacy and safety.
4. Research on anti-drug antibodies, PEG immunogenicity, and next-generation uricase platforms.