Recombinant Human Hyaluronidase in Subcutaneous Drug Delivery: Mechanism, Applications, and Development Considerations
Technical White Paper on rHuPH20-Enabled Subcutaneous Administration of Biologics and Large-Volume Formulations
Abstract
Subcutaneous (SC) drug delivery offers significant advantages over intravenous (IV) administration, including reduced healthcare burden, improved patient compliance, and the potential for home-based therapy. However, the extracellular matrix component hyaluronan creates a viscoelastic barrier in the hypodermis that restricts large-volume injection and slows the absorption of macromolecular therapeutics. This white paper examines the mechanism by which recombinant human hyaluronidase PH20 (rHuPH20) transiently degrades hyaluronan to facilitate SC administration of biologics, antibodies, and large-volume formulations. We analyze the enzymatic mechanism, current clinical applications including the ENHANZE® drug delivery platform, formulation development considerations, preclinical study design principles, and immunogenicity profiles. The data demonstrate that rHuPH20 enables SC delivery of therapeutic volumes up to 600 mL while maintaining comparable pharmacokinetic profiles to IV administration, with a modest immunogenicity incidence of 2–18% and no observed neutralizing antibodies across clinical trials.
recombinant human hyaluronidase, human hyaluronidase, rHuPH20, subcutaneous drug delivery, ENHANZE, biologics formulation
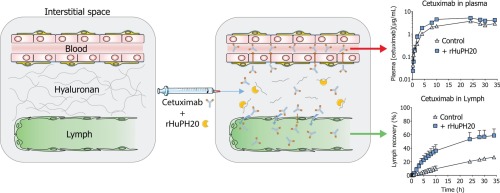
Fig 1. Mechanism of rHuPH20-facilitated subcutaneous drug delivery. (A) Native hyaluronan creates resistance to bulk fluid flow in the SC space. (B) rHuPH20 enzymatically depolymerizes hyaluronan. (C) Increased tissue permeability facilitates dispersion and absorption of co-administered therapeutics.
1. Executive Summary: Why Human Hyaluronidase Is Relevant to Subcutaneous Delivery
The transition from intravenous to subcutaneous drug delivery represents one of the most significant paradigm shifts in modern biotherapeutics administration. SC injection offers reduced infusion-related reactions, elimination of IV line placement, shorter administration times, and the potential for patient self-administration at home. However, physiological barriers in the subcutis—primarily the glycosaminoglycan hyaluronan—have historically limited SC delivery to small volumes (<2 mL) and small molecules.
Recombinant human hyaluronidase PH20 (rHuPH20) addresses this limitation by transiently degrading hyaluronan in the extracellular matrix, creating a window of enhanced tissue permeability that permits administration volumes up to 600 mL and improves the bioavailability of macromolecular therapeutics including monoclonal antibodies and immunoglobulins.
| Parameter | Traditional SC Delivery | rHuPH20-Enabled SC Delivery | IV Delivery |
|---|---|---|---|
| Maximum single-injection volume | 1–2 mL | Up to 600 mL | Unlimited (infusion) |
| Typical administration time | Minutes | 5–15 minutes | 1–4 hours |
| Macromolecular bioavailability | 50–70% | 80–100% | 100% |
| Patient setting | Home/Clinic | Home/Clinic | Hospital/Infusion center |
| Infusion reactions | Rare | Low | Moderate–High |
2. Hyaluronan and the Subcutaneous Tissue Barrier
2.1 Biophysical Properties of Hyaluronan
Hyaluronan (HA) is a high-molecular-weight glycosaminoglycan (typically 106–107 Da) composed of repeating disaccharide units of N-acetylglucosamine and glucuronic acid. In the subcutaneous interstitium, HA exists as a hydrated gel matrix intertwined with collagen fibrils, creating a viscoelastic barrier with two critical properties that limit drug delivery:
- High water-binding capacity: HA can bind up to 1,000 times its weight in water, creating substantial resistance to bulk fluid flow.
- Molecular sieving effect: The dense extracellular matrix restricts the diffusion of macromolecules >16 kDa, impeding absorption of therapeutic proteins and antibodies.
The concentration of HA in human subcutaneous tissue ranges from 0.5–2.5 mg/g wet weight, with higher concentrations in the dermal-epidermal junction. This distribution creates a physiological “bottleneck” that limits both the volume that can be administered and the rate at which large molecules access the systemic circulation.
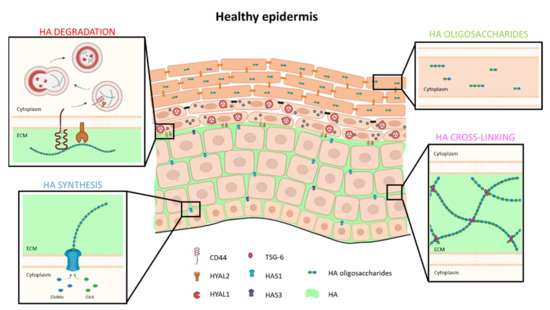
Fig 2. Distribution of hyaluronan in human skin and subcutaneous tissue. HA is concentrated in the papillary dermis and subcutaneous interstitium, where it forms a viscoelastic gel that restricts fluid flow and macromolecular diffusion.
2.2 Physiological Turnover and Regeneration
A critical advantage of targeting HA for drug delivery enhancement is its rapid physiological turnover. Unlike collagen or elastin, HA has a half-life of approximately 0.5 days in the skin and 2–3 days in the subcutis. Endogenous human hyaluronidases (Hyal-1, Hyal-2) continuously degrade and remodel the HA matrix. This natural turnover means that exogenous enzymatic degradation by rHuPH20 is fully reversible, with HA levels restoring to baseline within 24–48 hours post-injection.
3. rHuPH20 Mechanism of Action: Transient Degradation of Hyaluronan
3.1 Molecular Mechanism
rHuPH20 is a recombinant form of human sperm-associated antigen 1 (SPAM1/PH20), a glycosylphosphatidylinositol (GPI)-anchored hyaluronidase naturally expressed on the plasma membrane of sperm and mature macrophages. The therapeutic form lacks the GPI anchor domain, producing a soluble enzyme with specific activity 140- to 200-fold greater than animal-derived hyaluronidase preparations.
The enzymatic mechanism proceeds via hydrolysis of the β-1,4-glycosidic bond between N-acetylglucosamine and glucuronic acid residues. rHuPH20 functions as an endo-β-N-acetylhexosaminidase, cleaving high-molecular-weight HA into smaller oligosaccharides (primarily tetrasaccharides) that lose their water-retaining capacity and gel-forming properties.
Step 1: Injection and Dispersion — rHuPH20 is co-administered SC with the therapeutic agent (either sequentially or as a co-formulation).
Step 2: Enzymatic Degradation — rHuPH20 catalyzes the hydrolysis of HA in the interstitial matrix, reducing local viscosity.
Step 3: Enhanced Permeability — Reduced matrix resistance allows bulk fluid flow and macromolecular diffusion through expanded interstitial pathways.
Step 4: Absorption — Small molecules access capillaries; large proteins (>16 kDa) primarily drain into lymphatic vessels for systemic distribution.
Step 5: Matrix Restoration — Endogenous HA synthesis restores the native extracellular matrix within 24–48 hours.
3.2 Pharmacokinetic Impact
Clinical studies demonstrate that rHuPH20 co-administration significantly improves the pharmacokinetic profiles of SC-delivered therapeutics compared to SC administration without hyaluronidase:
| PK Parameter | Effect of rHuPH20 Co-administration | Clinical Significance |
|---|---|---|
| Bioavailability (F) | Increased to 80–100% | Achieves non-inferiority vs. IV route |
| Cmax | Increased by 1.5–3× | Higher peak concentrations |
| Tmax | Shortened by 30–50% | Faster onset of action |
| Intra-individual variability | Reduced CV by 20–40% | More predictable dosing |
| Injection site reactions | Reduced induration and pain | Improved tolerability |
rHuPH20 enables SC delivery of therapeutic volumes up to 600 mL while maintaining pharmacokinetic profiles comparable to IV administration. The enzymatic effect is localized to the injection site, with no detectable systemic exposure due to rapid clearance (terminal half-life of 5–6 minutes when administered IV).
4. Clinical Applications in Biologics and Large-Volume SC Injection
4.1 Approved Therapeutic Combinations
The ENHANZE® drug delivery platform (Halozyme Therapeutics) utilizes rHuPH20 to enable SC administration of previously IV-only therapeutics. Current FDA-approved combinations include:
| Product | Co-formulated Drug | Indication | SC Volume | Administration Time |
|---|---|---|---|---|
| HYLENEX® | rHuPH20 alone | SC hydration, drug dispersion | Variable | Minutes |
| Herceptin® SC | Trastuzumab | HER2+ breast cancer | 5 mL | 2–5 minutes |
| RITUXAN HYCELA® | Rituximab | Non-Hodgkin lymphoma, CLL | 11.7 mL | 5–7 minutes |
| HyQvia® | Human immunoglobulin (IGSC) | Primary immunodeficiency | 300–600 mL | 1–2 hours |
4.2 Application Categories
Monoclonal Antibodies: rHuPH20 facilitates SC delivery of full-length IgG antibodies (150 kDa) that would otherwise exhibit poor bioavailability via the SC route. The HannaH study demonstrated that trastuzumab SC plus rHuPH20 achieved non-inferior drug exposure (AUC) and comparable efficacy to IV trastuzumab, with patient preference strongly favoring the SC route (85% preference).
Immunoglobulin Replacement: For primary immunodeficiency, HyQvia® delivers 300–600 mL of 10% IgG solution subcutaneously every 3–4 weeks, compared to monthly IVIG infusions requiring 2–4 hours. The rHuPH20 component allows infusion rates of 300 mL/hour with reduced local adverse events compared to conventional SCIG.
High-Concentration Protein Formulations: Emerging applications include SC delivery of high-concentration (>200 mg/mL) monoclonal antibody formulations, where rHuPH20 mitigates injection site reactions and improves dispersion of viscous solutions.
5. Formulation Development Considerations
5.1 pH and Buffer System Optimization
The activity of rHuPH20 is highly dependent on environmental pH. The enzyme exhibits optimal activity between pH 6.0–7.0, with activity declining sharply below pH 5.0 and above pH 8.0. This pH dependency creates formulation constraints when co-formulating with therapeutic proteins that may require different pH environments for stability.
| Formulation Parameter | Optimal Range for rHuPH20 | Compatibility Considerations |
|---|---|---|
| pH | 6.0–7.0 | Must balance with therapeutic protein stability window |
| Buffer system | Histidine, phosphate | Avoid citrate buffers (>10 mM) which inhibit activity |
| Ionic strength | 100–200 mM | High salt can reduce enzymatic efficiency |
| Temperature | 2–8°C (storage) | Room temperature acceptable for administration |
| Protein concentration | Not limiting | High viscosity may require rHuPH20 dose adjustment |
5.2 Protein Stability and Compatibility
Co-formulation or sequential administration requires careful evaluation of protein-protein interactions between rHuPH20 and the therapeutic agent. Key considerations include:
- Aggregation potential: rHuPH20 is a glycoprotein with extensive N-linked glycosylation that minimizes self-association, but formulation screens should assess aggregate formation in mixed solutions.
- Shelf-life stability: Lyophilized or liquid co-formulations must demonstrate >24-month stability at 2–8°C with maintenance of both enzymatic activity and therapeutic protein potency.
- Container closure: Siliconized syringes and stoppers may affect rHuPH20 recovery; compatibility studies should include relevant delivery devices.
5.3 Excipient Selection
Formulation excipients must be selected to maintain both rHuPH20 activity and therapeutic protein integrity:
- Stabilizers: Sucrose, trehalose, and sorbitol are compatible with rHuPH20 and commonly used for protein stabilization.
- Surfactants: Polysorbate 20/80 (0.01–0.05%) are acceptable; avoid benzyl alcohol which can denature the enzyme.
- Amino acids: Arginine and histidine serve dual roles as buffers and stabilizers.
- Chelating agents: EDTA should be avoided as divalent cations (Ca2+, Mg2+) are required for optimal enzymatic activity.
Conduct orthogonal stability studies assessing both rHuPH20 enzymatic activity (via microtiter-based HA substrate assay) and therapeutic protein quality attributes (SEC-HPLC, potency) under accelerated and long-term storage conditions.
6. Preclinical and Translational Study Design
6.1 Species Selection and Model Validation
Preclinical evaluation of rHuPH20-enabled formulations requires careful species selection due to differences in skin architecture and HA distribution:
| Species | Skin HA Content | Translational Relevance | Primary Use Case |
|---|---|---|---|
| Miniature pig | High; similar to human | Gold standard for SC delivery | PK/PD, local tolerance |
| Cynomolgus monkey | Moderate | Regulatory toxicology standard | Safety assessment, ADA |
| Rabbit | Moderate | Historical hyaluronidase model | Enzymatic activity, local effects |
| Mouse | Low | Limited translational value | Mechanistic studies only |
6.2 Critical Study Endpoints
Preclinical programs should evaluate:
- Pharmacokinetic equivalence: Demonstrate AUC and Cmax non-inferiority vs. IV reference using validated bioanalytical methods.
- Local tissue effects: Histopathological assessment of injection sites at 24, 48, and 72 hours post-dose to confirm HA restoration and absence of chronic inflammation.
- Immunogenicity screening: Anti-rHuPH20 antibody detection using validated bridging immunoassays; assessment of neutralizing potential.
- Pharmacodynamic markers: For oncology applications, confirm equivalent receptor occupancy and downstream signaling inhibition.
- Drug product compatibility: In-use stability studies simulating patient handling conditions.
6.3 Dose Selection for rHuPH20
The rHuPH20 dose is typically fixed based on the volume of co-administered therapeutic rather than body weight. Standard dosing employs 1,000–2,000 U per mL of SC fluid, with a minimum of 6,000 U for volumes <6 mL. Dose-ranging studies should assess the minimum effective dose that achieves complete HA degradation in the injection depot without excessive enzyme load that could increase immunogenicity risk.
7. Safety and Immunogenicity Considerations
7.1 Clinical Immunogenicity Profile
Comprehensive immunogenicity assessment across 1,526 subjects in ten clinical trials reveals that rHuPH20 induces modest antibody responses with no observed impact on safety or efficacy:
| Immunogenicity Parameter | Observation | Clinical Implication |
|---|---|---|
| Baseline prevalence (pre-existing antibodies) | 3–12% across trials (5.8% in healthy donors) | Natural immune reactivity to PH20 epitopes |
| Treatment-induced incidence | 2–18% (varies by indication) | Highest in primary immunodeficiency (18.1%) |
| Neutralizing antibodies | 0% across all trials | No risk of loss of enzymatic efficacy |
| Titer magnitude (treatment-induced) | Median fold-change: 2×; rarely >10,000 | Generally transient, low-magnitude responses |
| Association with adverse events | No correlation observed | ADA positivity does not increase AE rates |
7.2 Antibody Characterization
Affinity-purified anti-rHuPH20 antibodies from both baseline-positive and treatment-induced subjects share similar characteristics:
- Isotype distribution: Predominantly IgG1 and IgG4 subclasses, indicating T-cell-dependent immune responses.
- Cross-reactivity: Binding to endogenous PH20 observed in vitro, but no functional consequence due to restricted tissue expression (testis/epididymis) and blood-tissue barriers.
- Paralog specificity: No cross-reactivity with Hyal-1, Hyal-2, or other hyaluronidase family members (34–42% homology).
No neutralizing antibodies were detected in any clinical trial, and there was no association between anti-rHuPH20 antibody positivity and local or systemic adverse events. The highest titers (>5,000) were observed in primary immunodeficiency patients receiving frequent IgG co-administration, but these titers diminished over time despite continued treatment.
7.3 Safety Monitoring Recommendations
Based on the clinical immunogenicity profile, routine safety monitoring should include:
- Baseline anti-rHuPH20 antibody screening (optional, given lack of clinical correlation).
- Periodic immunogenicity sampling in long-term studies (e.g., every 6–12 months).
- Standardized assessment of injection site reactions (ISR) using validated scales.
- Monitoring for hypersensitivity reactions, particularly in patients with history of allergic responses.
8. Future Directions: High-Concentration Protein Drugs and Combination Delivery Systems
8.1 High-Concentration Protein Drugs
The next generation of SC biologics targets concentrations >200 mg/mL to deliver therapeutic doses in volumes <5 mL. At these concentrations, protein solutions exhibit non-Newtonian viscosity and increased injection force. rHuPH20 addresses these challenges by:
- Reducing interstitial resistance to compensate for high formulation viscosity.
- Enabling dispersion of concentrated depot formations that would otherwise cause local inflammation.
- Permitting larger gauge needles (25G vs. 21G) by reducing required injection force.
8.2 Combination and Sequential Delivery Platforms
Emerging delivery strategies include:
| Platform Approach | Description | Development Stage |
|---|---|---|
| Co-formulated fixed-dose combinations | rHuPH20 and therapeutic protein in single vial | Marketed (Herceptin SC, RITUXAN HYCELA) |
| Sequential dual-cartridge devices | Auto-injectors delivering rHuPH20 followed by drug | Phase III |
| On-body infusion systems | Wearable pumps for large-volume SC delivery (>50 mL) | Phase II |
| Extended-release depots | rHuPH20 combined with sustained-release formulations | Preclinical |
8.3 Expansion to New Therapeutic Areas
Beyond oncology and immunology, rHuPH20-enabled delivery is being explored for:
- Neurology: SC administration of anti-CGRP antibodies for migraine prophylaxis.
- Dermatology: Enhanced delivery of biologics for psoriasis and atopic dermatitis.
- Endocrinology: Improved absorption of peptide hormones (e.g., GLP-1 agonists).
- Emergency medicine: Rapid SC fluid resuscitation in resource-limited settings.
8.4 Next-Generation Hyaluronidase Engineering
Protein engineering efforts are focused on developing hyaluronidase variants with:
- Extended enzymatic half-life for prolonged permeability windows.
- Reduced immunogenicity through glycoengineering or deimmunization.
- Targeted activity via conjugation to tissue-specific ligands.
- Thermostability for room-temperature storage and tropical climate distribution.
As the biopharmaceutical industry continues its shift toward patient-centric delivery models, rHuPH20-enabled subcutaneous administration will play an increasingly critical role in enabling the SC transition for established IV therapies and unlocking the potential of next-generation high-concentration biologics.
References
1. Bookbinder LH, Hofer A, Haller MF, et al. A recombinant human enzyme for enhanced interstitial transport of therapeutics. J Control Release. 2006;114(2):230-241.
2. Frost GI. Recombinant human hyaluronidase (rHuPH20): an enabling platform for subcutaneous drug and fluid administration. Expert Opin Drug Deliv. 2007;4(4):427-440.
3. Thomas J, von Hobe C, Muller R, et al. Comparative histology of mouse, pig, and human skin after intradermal and subcutaneous rHuPH20 injection. Int J Toxicol. 2009;28(5):401-409.
4. Wasserman RL, Melamed I, Kobrynski L, et al. Recombinant human hyaluronidase-facilitated subcutaneous immunoglobulin infusion in primary immunodeficiency diseases. J Clin Immunol. 2012;32(5):1036-1045.
5. Kang JS, DeLucia D, Cicalese R, et al. Subcutaneous dosing of co-formulated rHuPH20 and reference products: Comparative nonclinical assessment. J Pharm Sci. 2013;102(9):3269-3281.
6. Jackisch C, Hegg R, Vallentin S, et al. HannaH phase III randomized study: Subcutaneous trastuzumab with rHuPH20 versus intravenous trastuzumab in HER2-positive early breast cancer. Ann Oncol. 2015;26(Suppl 5):v1-v41.
7. Clinical immunogenicity of rHuPH20, a hyaluronidase enabling subcutaneous drug administration. AAPS J. 2015;17(4):948-957.
8. ENHANZE® drug delivery technology: A novel approach to subcutaneous administration using recombinant human hyaluronidase PH20. Drug Deliv. 2018;25(1):98-106.
9. European Medicines Agency. Assessment report for RITUXAN HYCELA. EMA/CHMP/484433/2017. 2018.
10. US Food and Drug Administration. Guidance for Industry: Immunogenicity Testing of Therapeutic Protein Products — Developing and Validating Assays for Anti-Drug Antibody Detection. 2019.