Recombinant Human Hyaluronidase and Subcutaneous Biologic Formulation
Opportunities and Challenges in High-Concentration Subcutaneous Delivery
Abstract
The shift from intravenous (IV) to subcutaneous (SC) administration represents one of the most significant trends in biologic drug development. While SC delivery offers substantial benefits in terms of patient convenience, healthcare resource utilization, and quality of life, the physical barriers of the subcutis—particularly the hyaluronan-rich extracellular matrix—limit injection volume and drug absorption rate. Recombinant human hyaluronidase PH20 (rHuPH20) has emerged as a transformative excipient that transiently degrades hyaluronan in the interstitial space, enabling large-volume SC injections (up to 10–15 mL) and accelerating the dispersion and absorption of co-administered biologics. This review systematically examines the expanding landscape of SC biologics, the barriers to large-volume SC delivery, the mechanistic role of rHuPH20 in modulating interstitial resistance, and the critical formulation, device, translational, and regulatory considerations that define successful co-formulation strategies. We also address persistent challenges including immunogenicity, inter-patient variability, and patient-specific factors, and offer a forward-looking perspective on next-generation SC delivery platforms.
recombinant human hyaluronidase biologics, subcutaneous formulation, high concentration biologics, hyaluronan, extracellular matrix, large-volume injection, co-formulation, immunogenicity
1. Why Subcutaneous Biologics Are Expanding
The biopharmaceutical industry has witnessed a pronounced paradigm shift toward subcutaneous delivery over the past two decades. Approximately 15 monoclonal antibody (mAb) products and numerous fusion proteins are now available in SC formulations, with many more in clinical development. This expansion is driven by a convergence of clinical, economic, and patient-centered factors.
From a clinical perspective, SC administration eliminates the need for vascular access, reducing the risk of catheter-related infections, thrombophlebitis, and infusion reactions. Patients with chronic conditions requiring frequent dosing—such as rheumatoid arthritis, multiple sclerosis, and primary immunodeficiency—benefit from the ability to self-administer at home, thereby reducing clinic visits and improving treatment adherence. Pharmacoeconomic analyses consistently demonstrate that SC biologics lower total healthcare costs by minimizing infusion center overhead, nursing time, and travel burden.
Technological advances have further catalyzed this transition. The development of high-concentration protein formulations (100–200 mg/mL), improved injection devices (autoinjectors, prefilled syringes, and wearable injectors), and the advent of recombinant human hyaluronidase as a permeation enhancer have collectively expanded the feasibility of SC delivery for biologics historically restricted to the intravenous route.
Table 1: Comparative overview of IV versus SC administration for biologic therapeutics.
| Factor | Intravenous (IV) | Subcutaneous (SC) |
|---|---|---|
| Administration Setting | Hospital / Infusion center | Home / Self-administration |
| Injection Volume | 50–500 mL (diluted) | 1–2 mL (standard); 10–15 mL (with rHuPH20) |
| Time per Dose | 1–4 hours | Seconds to minutes |
| Patient Convenience | Low (travel, scheduling) | High (flexible timing) |
| Healthcare Cost | Higher (facility, staff) | Lower (reduced overhead) |
| Immunogenicity Risk | Lower (gradual exposure) | Higher (depot effect, aggregates) |
2. Barriers to Large-Volume Subcutaneous Delivery
Despite the compelling advantages of SC delivery, the subcutis presents formidable physical and physiological barriers that constrain the volume, viscosity, and molecular weight of injectable biologics.
2.1 The Hyaluronan Barrier
The interstitial matrix of the hypodermis is densely populated with hyaluronan (HA), a high-molecular-weight glycosaminoglycan (typically 10⁶–10⁷ Da) that forms a viscoelastic gel network. Hyaluronan occupies the spaces between collagen fibrils and elastin fibers, creating a hydrodynamic resistance that limits bulk fluid flow. Under normal conditions, the subcutis can accommodate only 1–2 mL of injected fluid before tissue turgor pressure rises sharply, causing pain, leakage, and incomplete absorption.
Hyaluronan is not merely a passive structural element; it actively regulates interstitial fluid pressure, water homeostasis, and the trafficking of macromolecules. Its high negative charge density attracts cations and water, generating significant osmotic pressure. For large therapeutic proteins (>100 kDa), the effective pore size of the HA–collagen network acts as a size-exclusion barrier, slowing diffusion and favoring lymphatic uptake over direct capillary absorption.
2.2 Viscosity and Concentration Limits
High-concentration protein formulations (>150 mg/mL) exhibit non-Newtonian shear-thinning behavior and elevated viscosity (often >20 cP), which complicates injection through fine-gauge needles (25G–27G). High viscosity increases injection force requirements, prolongs administration time, and raises the risk of needle clogging or breakage. Formulators must balance the need for high protein concentration (to keep injection volume manageable) against the physical limits of injectability and patient comfort.
2.3 Pain and Tolerability Thresholds
Patient acceptance of SC injection is strongly influenced by pain perception, which is affected by injection volume, flow rate, formulation osmolality, pH, and buffer composition. Volumes exceeding 2 mL per injection site typically elicit discomfort and are associated with higher rates of injection-site reactions (erythema, edema, induration). For chronic therapies requiring frequent administration, cumulative tissue damage and lipohypertrophy at repeated injection sites further compromise long-term tolerability.
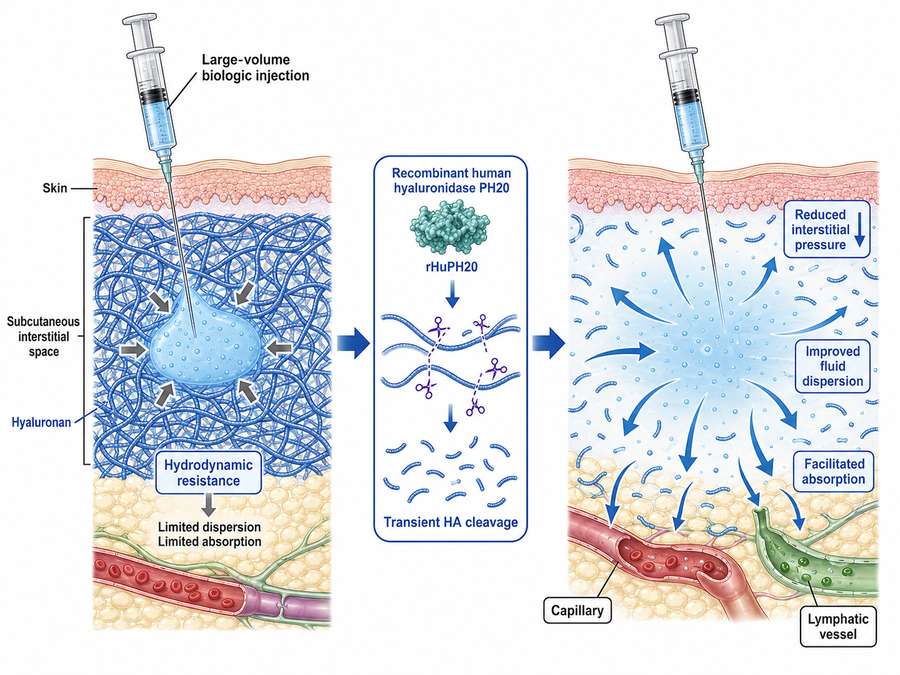
Fig 1. Schematic illustration of the subcutaneous extracellular matrix barrier. Hyaluronan (blue filaments) forms a dense meshwork within the interstitial space, creating hydrodynamic resistance that limits the dispersion and absorption of large-volume biologic injections. Recombinant human hyaluronidase PH20 transiently cleaves hyaluronan, reducing interstitial pressure and facilitating fluid dispersion.
3. Role of rHuPH20 in Modulating Interstitial Resistance
3.1 Enzymatic Mechanism and Kinetics
Recombinant human hyaluronidase PH20 (rHuPH20) is a soluble, neutral-active enzyme derived from the human sperm adhesion molecule 1 (SPAM1) gene product. It catalyzes the hydrolysis of the β-1,4-glycosidic bond between N-acetylglucosamine and D-glucuronic acid residues in hyaluronan, effectively depolymerizing the high-molecular-weight polymer into smaller oligosaccharides. Unlike the crude bovine or ovine hyaluronidase preparations used historically, rHuPH20 is produced in Chinese hamster ovary (CHO) cells and exhibits high specific activity, batch consistency, and a favorable safety profile.
The enzymatic activity of rHuPH20 is optimal at neutral pH (6.5–7.5), which aligns well with the pH of most biologic formulations (pH 5.0–7.0). Upon SC co-injection, rHuPH20 acts locally and transiently: it begins cleaving hyaluronan within minutes, reaches peak activity within 1–2 hours, and allows endogenous hyaluronan to regenerate fully within 24–48 hours. This transient action is critical because it avoids permanent structural damage to the extracellular matrix while creating a temporary window of enhanced permeability.
3.2 Impact on Injection Volume and Absorption Kinetics
Clinical and preclinical studies have consistently demonstrated that co-formulation with rHuPH20 increases the maximum feasible SC injection volume from approximately 2 mL to 10–15 mL per site. This volume expansion is achieved through a reduction in interstitial fluid pressure and an increase in the effective hydraulic conductivity of the subcutis. The depolymerized hyaluronan fragments are cleared via lymphatic drainage, and the restored matrix architecture supports repeated dosing without cumulative tissue damage.
Importantly, rHuPH20 does not compromise the pharmacokinetic (PK) profile of the co-administered biologic. In fact, by promoting more uniform dispersion across a larger tissue area, rHuPH20 can reduce local peak concentrations and smooth the absorption profile. Bioavailability of co-formulated mAbs typically ranges from 50% to 80% relative to IV administration, with time-to-peak concentration (Tmax) occurring between 2 and 5 days—an acceptable trade-off for the convenience of SC delivery.
Table 2: Comparative impact of rHuPH20 co-formulation on subcutaneous delivery parameters.
| Parameter | Without rHuPH20 | With rHuPH20 |
|---|---|---|
| Max Injection Volume per Site | 1–2 mL | 10–15 mL |
| Hyaluronan Half-Life (Local) | ~24–48 hours (natural turnover) | < 1 hour (accelerated degradation) |
| Matrix Recovery Time | N/A | 24–48 hours |
| Biologic Bioavailability | 50–70% | 60–80% |
| Injection-Site Reaction Rate | Moderate to high (>2 mL) | Reduced (dispersed volume) |
| Need for Multiple Injection Sites | Common for doses >2 mL | Typically single site |
3.3 Approved and Pipeline Co-Formulations
The clinical validation of rHuPH20 co-formulation was established with the approval of Hylenex® (hyaluronidase human injection) and subsequently advanced through the Enhanze® drug delivery technology platform. Notable approved products include:
- Herceptin Hylecta® (trastuzumab + hyaluronidase-oysk): Approved for HER2-positive breast cancer, enabling a 5-minute SC injection versus the standard 30–90 minute IV infusion.
- Rituxan Hycela® (rituximab + hyaluronidase human): Approved for non-Hodgkin lymphoma and chronic lymphocytic leukemia, reducing infusion time from several hours to approximately 5–7 minutes.
- Darzalex Faspro® (daratumumab + hyaluronidase-fihj): Approved for multiple myeloma, offering a 3–5 minute SC injection as an alternative to the multi-hour IV infusion.
- Phesgo® (pertuzumab + trastuzumab + hyaluronidase-zzxf): A fixed-dose combination for HER2-positive breast cancer, administered SC in approximately 8 minutes.
The integration of recombinant human hyaluronidase into co-formulation strategies has reduced administration times from hours to minutes, fundamentally transforming the patient experience and healthcare delivery model for biologic cancer therapies.
4. Formulation Compatibility Considerations
Successful co-formulation of a biologic with rHuPH20 requires meticulous attention to physicochemical compatibility, as the enzyme, the therapeutic protein, and the excipient matrix must maintain stability and activity throughout shelf life and administration.
4.1 pH and Buffer Compatibility
rHuPH20 exhibits optimal enzymatic activity at neutral pH, with a sharp decline in activity below pH 5.5 and above pH 8.0. Many mAb formulations are buffered in the pH 5.0–6.0 range to maximize protein solubility and minimize chemical degradation (e.g., asparagine deamidation, methionine oxidation). This pH mismatch presents a formulation challenge: the co-formulation must either operate at a compromise pH (typically 5.5–6.5) where both the mAb and rHuPH20 retain acceptable stability, or employ a dual-chamber device that keeps the components separate until injection.
Histidine and phosphate buffers are commonly employed due to their buffering capacity in the relevant range and their compatibility with both proteins. Citrate buffers, while popular in IV formulations, may chelate metal ions required for rHuPH20 activity and are generally avoided in co-formulations.
4.2 Ionic Strength and Osmolality
Ionic strength modulates both protein–protein interactions and enzyme kinetics. High salt concentrations (>300 mM) can screen electrostatic interactions, promoting protein aggregation, while also altering the conformational dynamics of rHuPH20. Osmolality must be maintained within the physiological range (250–350 mOsm/kg) to minimize pain upon injection and prevent tissue irritation. Hyperosmolar formulations (>600 mOsm/kg) are associated with stinging sensations and local inflammation, whereas hypoosmolar solutions can cause cell lysis.
4.3 Surfactants and Stabilizers
Polysorbate 20 and Polysorbate 80 are standard surfactants in biologic formulations, protecting against interfacial stress and aggregation. However, surfactants can interact with hydrophobic patches on rHuPH20, potentially affecting its activity or stability. Polyethylene glycol (PEG) and amino acids such as arginine, histidine, and proline are frequently used as stabilizers and viscosity reducers in high-concentration formulations. The compatibility of these excipients with rHuPH20 must be confirmed through accelerated stability studies and activity assays.
4.4 Preservatives and Antimicrobial Agents
Multi-dose formulations require antimicrobial preservatives such as benzyl alcohol or phenol. These agents can denature proteins and inhibit enzyme activity. For rHuPH20 co-formulations, single-use vials or prefilled syringes are generally preferred to eliminate the need for preservatives, thereby simplifying compatibility assessments and reducing safety concerns.
5. Protein Stability and Excipient Screening
High-concentration protein formulations (>100 mg/mL) are inherently prone to physical and chemical instability, and the addition of rHuPH20 introduces another macromolecular component that can participate in deleterious interactions.
5.1 Aggregation Pathways
At elevated concentrations, protein–protein interactions become favorable, leading to reversible self-association and, ultimately, irreversible aggregation. The presence of rHuPH20 can influence this behavior through excluded volume effects, electrostatic interactions, and transient binding. Size-exclusion chromatography (SEC), analytical ultracentrifugation (AUC), and dynamic light scattering (DLS) are essential tools for monitoring aggregate formation in co-formulations.
Thermal stress studies (e.g., 40°C for 1–3 months) and freeze–thaw cycling are standard methods for assessing formulation robustness. Co-formulations must demonstrate that rHuPH20 does not accelerate the aggregation kinetics of the therapeutic protein and that the therapeutic protein does not inhibit rHuPH20 enzymatic activity.
5.2 Chemical Degradation
Chemical degradation pathways—including asparagine deamidation, aspartic acid isomerization, methionine oxidation, and disulfide bond scrambling—are influenced by formulation pH, buffer composition, and the presence of reactive species. rHuPH20 contains multiple methionine and cysteine residues that are susceptible to oxidation, necessitating the exclusion of reactive oxygen species and the potential inclusion of antioxidants such as methionine or sodium thiosulfate.
5.3 Excipient Screening Strategy
A systematic excipient screening approach typically employs a design-of-experiments (DoE) framework to evaluate the individual and synergistic effects of buffers, salts, sugars, amino acids, and surfactants. Key response variables include:
- Physical stability: Monomer content by SEC, subvisible particle count by micro-flow imaging (MFI), opalescence by turbidimetry.
- Chemical stability: Charge variant profile by ion-exchange chromatography (IEX) or imaged capillary isoelectric focusing (icIEF), oxidation levels by peptide mapping.
- rHuPH20 activity: Enzymatic activity assay using a turbidimetric or colorimetric substrate (e.g., hyaluronan incubation followed by measurement of reducing ends).
- Biologic potency: Cell-based assay or binding assay to confirm maintenance of therapeutic activity.
Table 3: Excipient compatibility considerations for rHuPH20 co-formulations.
| Excipient Class | Examples | Function | Compatibility Notes with rHuPH20 |
|---|---|---|---|
| Buffer | Histidine, Phosphate | pH control | Histidine preferred; avoid citrate (metal chelation) |
| Tonicity Agent | NaCl, Sucrose, Trehalose | Osmolality adjustment | Generally compatible; high NaCl may affect enzyme kinetics |
| Surfactant | Polysorbate 20, Polysorbate 80 | Interfacial stabilization | Verify no inhibition of rHuPH20 activity |
| Viscosity Reducer | Arginine HCl, Proline | Reduce injection force | Compatible; may enhance protein solubility |
| Antioxidant | Methionine, Sodium Thiosulfate | Prevent oxidation | Recommended for rHuPH20 cysteine/methionine protection |
| Chelator | EDTA | Metal ion control | Use cautiously; may inhibit rHuPH20 metal-dependent activity |
6. Device and Injection Volume Considerations
The delivery device is an integral component of the SC biologic product, influencing dosing accuracy, patient experience, and clinical outcomes. The choice of device must align with the formulation properties (viscosity, volume) and the target patient population.
6.1 Prefilled Syringes and Autoinjectors
For volumes up to 2 mL, prefilled syringes (PFS) and autoinjectors (AI) represent the gold standard in patient-centric design. These devices conceal the needle, control injection speed, and incorporate safety features to prevent needlestick injuries. However, standard PFS/AI systems are not designed for the higher injection forces required by viscous, large-volume formulations.
6.2 Large-Volume Wearable Injectors
Wearable injectors (also known as on-body delivery systems, OBDS) have emerged as a solution for volumes exceeding 3–5 mL. These adhesive patch-like devices are applied to the abdomen or thigh and deliver the drug over several minutes to hours via a subcutaneous cannula. While OBDS enable large-volume SC delivery without rHuPH20, they add complexity, cost, and training requirements. The combination of rHuPH20 with a standard PFS or AI offers a simpler, more cost-effective alternative for volumes in the 5–15 mL range.
6.3 Needle Gauge and Length
Needle selection balances patient comfort (finer gauges reduce pain) with injectability (wider gauges reduce resistance). For high-concentration, high-viscosity formulations, 25G–27G needles with lengths of ½ inch (12.7 mm) to ⅝ inch (16 mm) are standard. The needle length must be sufficient to reach the subcutaneous fat layer without penetrating into muscle, which would alter absorption kinetics.
6.4 Injection Speed and Force
Injection speed directly correlates with tissue distension and pain perception. Autoinjectors are engineered to deliver the full dose within 10–15 seconds for standard volumes, but large-volume injections may require 30–60 seconds to remain within acceptable force limits. Formulators must characterize the force–velocity profile of the formulation to ensure compatibility with the chosen device spring mechanism.
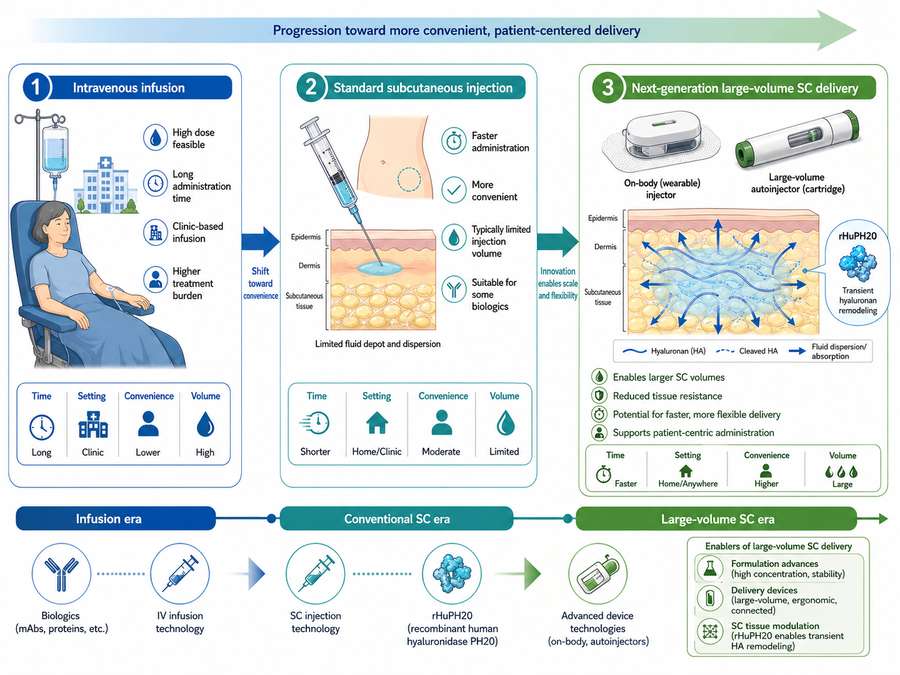
Fig 2. Development roadmap for subcutaneous delivery of high-dose biologics, illustrating the progression from intravenous infusion to standard subcutaneous injection and next-generation large-volume SC delivery enabled by rHuPH20 and advanced device technologies.
7. Translational and Regulatory Considerations
The transition from IV to SC administration, particularly with the incorporation of a novel excipient such as recombinant human hyaluronidase, triggers a comprehensive regulatory framework that encompasses pharmacology, toxicology, clinical efficacy, and quality control.
7.1 Bridging Studies and Bioequivalence
Regulatory agencies (FDA, EMA, PMDA) require robust evidence that the SC co-formulation achieves comparable exposure (AUC, Cmax) and pharmacodynamic response to the established IV product. This typically involves a Phase I comparative pharmacokinetic study in healthy volunteers or patients, followed by a Phase III efficacy and safety trial. The bioequivalence margin for AUC is generally set at 80–125%, although wider margins may be acceptable for certain indications if justified clinically.
7.2 Immunogenicity Assessment
The immunogenicity risk of the co-formulation must be evaluated for both the therapeutic protein and rHuPH20. Anti-drug antibody (ADA) assays must be capable of distinguishing antibodies directed against the biologic from those targeting rHuPH20. Neutralizing antibody (NAb) assays are particularly important for rHuPH20, as persistent NAbs could compromise the efficacy of subsequent doses and potentially cross-react with endogenous hyaluronidases (e.g., HYAL1, HYAL2), although clinical evidence for such cross-reactivity remains limited.
7.3 Quality Control and Release Specifications
The co-formulation requires a unified set of release specifications that cover identity, purity, potency, and safety for both components. Critical quality attributes (CQAs) include:
- rHuPH20 enzymatic activity: Measured in USP units/mg using a standardized substrate.
- Biologic potency: Cell-based or binding assay specific to the therapeutic mechanism.
- Aggregate content: SEC-HPLC with acceptance criteria typically set at <5% high-molecular-weight species.
- Subvisible particles: Measured by light obscuration or MFI; compliance with USP <788>.
- Endotoxin and bioburden: Standard LAL testing and sterility assurance.
7.4 Stability and Shelf Life
Real-time and accelerated stability studies must demonstrate that the co-formulation maintains all CQAs throughout the proposed shelf life (typically 18–36 months at 2–8°C). Freeze–thaw studies, photostability testing (ICH Q1B), and in-use stability studies (simulating patient handling conditions) are mandatory components of the regulatory dossier.
8. Challenges: Immunogenicity, Variability, and Patient Factors
Despite the clinical successes of rHuPH20-enabled SC biologics, several challenges persist that warrant careful consideration during development and post-market surveillance.
8.1 Immunogenicity of rHuPH20
As a foreign (albeit human-derived) protein administered repeatedly via the immunologically active subcutaneous route, rHuPH20 carries an inherent risk of eliciting an immune response. Clinical trials of rHuPH20 co-formulations have reported ADA incidence rates ranging from <1% to approximately 10%, depending on the patient population, dosing frequency, and assay sensitivity. The majority of ADAs are transient and low-titer, but persistent high-titer antibodies can neutralize rHuPH20 activity, reducing the efficiency of subsequent injections.
The theoretical concern of cross-reactivity with endogenous hyaluronidases (particularly HYAL1 and HYAL2, which are involved in tissue remodeling and glycosaminoglycan catabolism) has been investigated in nonclinical studies. To date, no clinical syndrome resembling hyaluronan storage disease has been reported in patients treated with rHuPH20, suggesting that the transient, local administration does not induce systemic pathological autoimmunity. Nonetheless, long-term pharmacovigilance remains essential.
8.2 Inter-Patient and Intra-Patient Variability
Subcutaneous absorption is influenced by a multitude of patient-specific factors, including body mass index (BMI), subcutaneous fat thickness, skin temperature, hydration status, and local blood flow. Obese patients may exhibit altered absorption kinetics due to differences in interstitial pressure and lymphatic drainage. Similarly, injection-site rotation (abdomen, thigh, upper arm) can introduce variability in bioavailability. Formulators and clinicians must account for this variability when designing dosing regimens and interpreting PK data.
8.3 Patient Education and Adherence
The transition to self-administered SC therapy places greater responsibility on patients for proper technique, storage, and adherence. Education programs must address injection-site rotation, recognition of adverse reactions, and the importance of compliance. For elderly patients or those with limited dexterity, caregiver training and device selection (e.g., larger grip surfaces, audible feedback) are critical determinants of successful therapy.
8.4 Cost and Reimbursement
While SC delivery reduces healthcare system costs, the addition of rHuPH20 and specialized devices can increase the drug product cost. Payers may require evidence of non-inferior clinical outcomes and improved quality-of-life metrics to justify reimbursement. Health technology assessment (HTA) bodies increasingly consider patient-reported outcomes (PROs) and real-world evidence (RWE) in their evaluations.
Immunogenicity remains the most significant long-term risk for rHuPH20 co-formulations. While current data suggest a favorable safety profile, the potential for neutralizing antibodies to compromise efficacy and cross-react with endogenous hyaluronidases necessitates rigorous post-market surveillance and the development of next-generation hypoimmunogenic enzyme variants.
9. Future Outlook
The field of SC biologic delivery is poised for continued innovation, driven by advances in protein engineering, formulation science, and device technology.
9.1 Next-Generation Hyaluronidase Variants
Protein engineering efforts are focused on developing rHuPH20 variants with reduced immunogenicity, enhanced enzymatic activity at acidic pH, and improved stability. Site-directed mutagenesis to eliminate immunodominant epitopes, coupled with PEGylation or glycoengineering to shield surface antigens, may yield "stealth" hyaluronidases that evade immune surveillance while maintaining robust catalytic function.
9.2 Sustained-Release SC Depots
Beyond immediate dispersion, researchers are exploring the use of hyaluronan-based hydrogels and in situ forming depots to achieve sustained-release SC delivery. By tuning the cross-linking density and degradation rate of the hydrogel, it may be possible to create a tunable release matrix that provides zero-order kinetics over weeks or months, reducing dosing frequency for chronic therapies.
9.3 Continuous Manufacturing and Real-Time Release
The adoption of continuous manufacturing (CM) for biologics offers opportunities to integrate formulation and filling in a seamless process, reducing batch-to-batch variability and enabling real-time release testing (RTRT). For co-formulations, CM could facilitate the precise blending of rHuPH20 and the therapeutic protein under controlled conditions, ensuring uniform activity distribution throughout the batch.
9.4 Personalized SC Delivery
The convergence of wearable sensors, artificial intelligence, and connected health platforms is enabling personalized SC delivery. Smart autoinjectors equipped with biometric sensors could adjust injection parameters (speed, depth, volume) based on real-time feedback from the tissue, optimizing absorption and minimizing discomfort for individual patients.
In conclusion, recombinant human hyaluronidase has fundamentally expanded the boundaries of subcutaneous biologic delivery, transforming patient care across oncology, immunology, and beyond. As formulation scientists, device engineers, and regulatory specialists continue to refine co-formulation strategies, the vision of universal, patient-friendly SC administration for all biologic therapeutics moves closer to reality. The challenges ahead—immunogenicity, variability, and cost—are substantial but surmountable, and the field stands at the threshold of a new era in drug delivery innovation.
References
1. Bookbinder, L. H., et al. (2006). A recombinant human enzyme for enhanced interstitial transport of therapeutics. J Control Release, 114(2): 230-241.
2. Dick, L. W., et al. (2019). Subcutaneous delivery of high-dose/volume biologics: Current status and prospect for large volume injection systems. Drug Deliv Transl Res, 9(4): 815-826.
3. Klinge, S. A., & Sawyer, G. A. (2013). Effectiveness and safety of topical hyaluronidase in treating skin injuries: A systematic review. J Drugs Dermatol, 12(12): 1402-1408.
4. Locke, K. W., et al. (2019). ENHANZE® drug delivery technology: A novel approach to subcutaneous administration using recombinant human hyaluronidase PH20. Drug Deliv, 26(1): 98-106.
5. Melani, A. S., & Bonavia, M. (2017). Subcutaneous administration of biologic agents in the treatment of inflammatory rheumatic diseases. Adv Ther, 34(4): 818-838.
6. Richter, A., & Anton, S. E. (2012). Patient preferences for route of administration: A systematic review. Patient, 5(3): 155-165.
7. Shpilberg, O., & Jackisch, C. (2013). Subcutaneous administration of rituximab (MabThera) and trastuzumab (Herceptin) using recombinant human hyaluronidase. Br J Cancer, 109(6): 1556-1561.
8. Stern, R. (2004). Hyaluronan catabolism: A new metabolic pathway. Eur J Cell Biol, 83(7): 317-325.
9. U.S. Food and Drug Administration. (2015). Guidance for Industry: Immunogenicity Assessment for Therapeutic Protein Products. FDA, Silver Spring, MD.
10. Waugh, W. J., et al. (2020). Formulation development of high-concentration monoclonal antibodies: A review of current strategies and challenges. J Pharm Sci, 109(1): 123-138.