Comparison of Enzyme Replacement Therapies for Gaucher Disease
Imiglucerase vs Velaglucerase vs Taliglucerase: Mechanistic and Clinical Perspectives
Abstract
Enzyme replacement therapy (ERT) has fundamentally transformed the management of Gaucher disease type 1 since the approval of alglucerase in 1991. Currently, three recombinant glucocerebrosidase products are available for clinical use: imiglucerase (Cerezyme), velaglucerase alfa (VPRIV), and taliglucerase alfa (Elelyso). While these therapeutics share a common mechanism of macrophage-targeted enzyme delivery via mannose receptor-mediated uptake, they differ significantly in manufacturing processes, glycosylation patterns, and immunogenicity profiles. This comparative analysis examines the structural, pharmacological, and clinical distinctions among these ERT options to inform therapeutic decision-making and research applications.
imiglucerase vs velaglucerase, Gaucher therapy comparison, enzyme replacement therapy, taliglucerase alfa, glucocerebrosidase deficiency
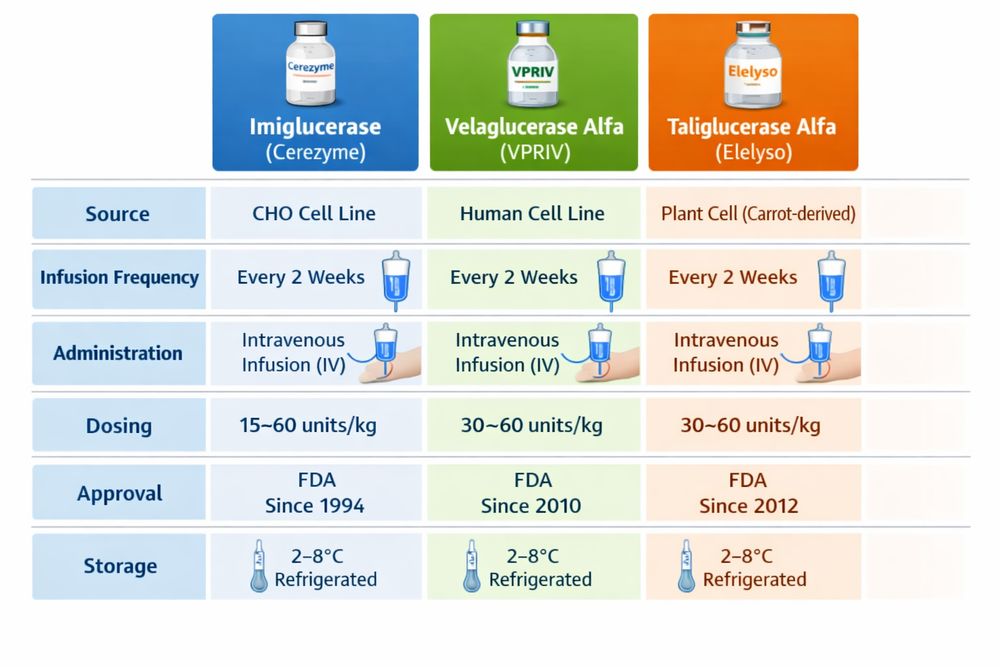
Fig 1. Comparative overview of enzyme replacement therapies for Gaucher disease
1. Overview of ERT Therapies
Gaucher disease type 1, the most prevalent lysosomal storage disorder, results from inherited deficiencies in glucocerebrosidase (GCase, acid β-glucosidase), leading to progressive accumulation of glucosylceramide within macrophage lysosomes. The introduction of ERT marked a paradigm shift from symptomatic management to disease-modifying intervention.
The first FDA-approved ERT, alglucerase (Ceredase), derived from human placenta and established proof-of-concept for enzyme supplementation strategies. However, limited tissue availability and infectious disease concerns necessitated transition to recombinant production systems. Today, clinicians may select from three distinct recombinant products, each utilizing different expression platforms and glycoengineering approaches to achieve macrophage targeting.
| Product | Brand Name | Manufacturer | Cell Expression System | FDA Approval |
|---|---|---|---|---|
| Imiglucerase | Cerezyme | Sanofi Genzyme | Chinese Hamster Ovary (CHO) | 1994 |
| Velaglucerase alfa | VPRIV | Takeda (Shire) | Human fibrosarcoma (HT-1080) | 2010 |
| Taliglucerase alfa | Elelyso | Protalix/Pfizer | Carrot cells (ProCellEx) | 2012 |
All three enzymes are administered via intravenous infusion every other week at standard doses of 60 U/kg, though individualized dosing based on therapeutic goals and patient response remains essential clinical practice.
2. Imiglucerase
Imiglucerase represents the benchmark against which newer ERTs are measured, with over three decades of clinical experience supporting its efficacy and safety profile. Produced in Chinese hamster ovary (CHO) cells, this recombinant enzyme incorporates a histidine substitution at amino acid residue 495 (rather than the wild-type arginine) and features enzymatically trimmed N-linked glycans terminating in exposed α-mannose residues to facilitate macrophage targeting.
2.1 Manufacturing and Structural Characteristics
The CHO cell expression system enables high-yield production of properly folded glucocerebrosidase with mammalian-compatible glycosylation patterns. Post-production processing involves enzymatic deglycosylation using exoglycosidases to expose terminal mannose residues, creating a uniform glycan structure optimized for binding to macrophage mannose receptors (CD206).
2.2 Clinical Efficacy Profile
Longitudinal data from the International Collaborative Gaucher Group (ICGG) Registry, encompassing over 5,000 patients, demonstrate consistent therapeutic responses:
- Hematologic improvements: Hemoglobin concentrations typically normalize within 6-12 months of initiation, with mean increases of approximately 1.9 g/dL sustained through 5 years of treatment.
- Visceral reductions: Liver volumes decrease by approximately 11% within 6 months, with progressive normalization over extended therapy.
- Splenic response: Spleen volume reduction occurs more gradually, with significant improvements observed over 24-48 months, particularly in patients with massive splenomegaly.
- Platelet recovery: Baseline-dependent improvements typically manifest within 12-24 months, correlating with splenic regression.
| Clinical Parameter | Typical Response | Time to Response |
|---|---|---|
| Hemoglobin increase | +1.9 g/dL (average) | 6-12 months |
| Liver volume reduction | ~11% decrease | 6 months |
| Platelet count improvement | Baseline-dependent | 12-24 months (with spleen) |
| Spleen volume reduction | Variable (dose-dependent) | 24-48 months |
Patients with intact spleens demonstrate slower platelet recovery compared to splenectomized patients, reflecting the pathophysiologic role of splenic sequestration in Gaucher disease thrombocytopenia.
3. Velaglucerase Alfa
Velaglucerase alfa (VPRIV) utilizes Gene-Activation technology in a human fibrosarcoma cell line (HT-1080), producing an enzyme with the wild-type amino acid sequence including arginine at position 495. Its glycosylation pattern differs fundamentally from imiglucerase: kifunensine inhibition during production yields high-mannose type oligosaccharides that are less extensively processed than the CHO-derived counterpart.
3.1 Comparative Clinical Evidence
Head-to-head clinical trials have established non-inferiority to imiglucerase. In the pivotal 9-month randomized trial (HGT-GCB-039), treatment-naïve patients receiving velaglucerase alfa demonstrated hemoglobin changes statistically equivalent to those receiving imiglucerase (mean difference: 0.14 g/dL; 95% CI: -0.57 to 0.84). Secondary endpoints including platelet counts, liver volumes, and spleen volumes showed no significant differences between treatment groups.
3.2 Distinctive Features in Imiglucerase vs Velaglucerase Comparison
| Characteristic | Imiglucerase | Velaglucerase Alfa |
|---|---|---|
| Amino acid 495 | Histidine | Arginine (wild-type) |
| Glycan structure | Trimmed (Man3GlcNAc2) | High-mannose (less processed) |
| Cell line | CHO | Human fibrosarcoma |
| Mannose content | ~3 residues | Higher natural content |
| IgG antibody formation | 13-15% in clinical trials | Lower rates observed |
Notably, the head-to-head trial revealed differential immunogenicity profiles: while no patients developed antibodies to velaglucerase alfa, 23.5% of imiglucerase-treated patients developed IgG antibodies cross-reactive with both enzymes. This distinction may influence therapy selection in patients with documented antibody formation or infusion-related reactions.
3.3 Switching Studies
Long-term extension studies support safe transition between products. Patients stable on imiglucerase who switched to velaglucerase alfa maintained hematologic and visceral parameters over 12-24 months, with trends toward improved platelet counts and biomarker reductions. These data support therapeutic flexibility in clinical practice.
4. Taliglucerase Alfa
Taliglucerase alfa (Elelyso) represents a paradigm shift in biopharmaceutical manufacturing as the first plant-cell-derived human recombinant enzyme approved for therapeutic use. Produced in carrot cells using Protalix's proprietary ProCellEx platform, this enzyme introduces unique structural considerations distinct from mammalian-cell-derived alternatives.
4.1 Structural Distinctions
Taliglucerase alfa contains plant-specific sequences: a 2-amino acid extension at the N-terminus and a 7-amino acid vacuolar targeting peptide at the C-terminus. These additions, absent in mammalian-cell-derived alternatives, initially raised immunogenicity concerns regarding plant-specific glycan epitopes (core α(1-2)-xylose and core α(1-3)-fucose). However, clinical experience has demonstrated manageable safety profiles with appropriate monitoring.
4.2 Clinical Performance Data
| Study Population | Dose | Key Efficacy Findings | Duration |
|---|---|---|---|
| Treatment-naïve adults | 30 U/kg | 50.1% spleen volume reduction | 36 months |
| Treatment-naïve adults | 60 U/kg | 64.6% spleen volume reduction | 36 months |
| Cerezyme-switch patients | Comparable dosing | Maintained clinical stability | 24+ months |
Common adverse reactions include headache, arthralgia, fatigue, and nausea, with hypersensitivity reactions requiring standard infusion precautions and premedication protocols similar to other ERT products.
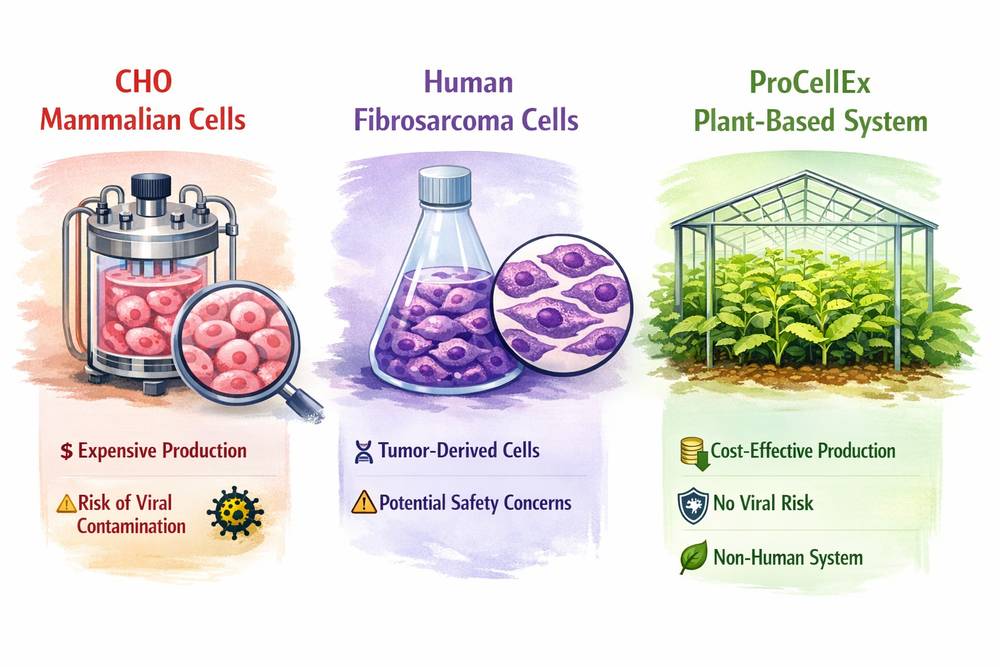
Fig 2. Manufacturing platform comparison: Mammalian CHO cells, human fibrosarcoma cells, and plant-based ProCellEx system
5. Mechanistic Differences
While all three ERTs catalyze glucocerebroside hydrolysis to glucose and ceramide within macrophage lysosomes, subtle mechanistic variations influence their pharmacological behavior and therapeutic characteristics.
5.1 Manufacturing and Glycosylation Impact on Targeting
Imiglucerase undergoes post-production enzymatic deglycoslation to expose terminal mannose residues, creating a uniform but artificially modified glycan structure optimized for macrophage mannose receptor binding.
Velaglucerase alfa leverages kifunensine-mediated pathway inhibition to preserve high-mannose structures naturally, potentially offering enhanced receptor affinity due to increased mannose density and less processed glycan chains.
Taliglucerase alfa utilizes the plant vacuolar sorting pathway, where endogenous plant mannosidases expose terminal mannose residues without requiring exogenous enzymatic treatment, though with plant-specific glycan modifications.
5.2 Tissue Distribution Patterns
Preclinical studies in Gaucher mouse models demonstrate comparable tissue distribution across products: approximately 80% of administered enzyme localizes to liver interstitial cells, with less than 5% reaching spleen and lungs after intravenous bolus injection. Both imiglucerase and velaglucerase alfa showed dose-dependent reductions in glucosylceramide levels (60-95% in liver, 10-30% in spleen), though velaglucerase alfa demonstrated slightly faster hepatic glucosylceramide reduction at 60 U/kg/week at the 4-week timepoint.
5.3 Comparative Pharmacological Properties
| Property | Imiglucerase | Velaglucerase Alfa | Taliglucerase Alfa |
|---|---|---|---|
| Production system | Mammalian (CHO) | Human cell line | Plant (carrot) |
| Glycan processing | Ex vivo enzymatic | In vivo pathway inhibition | Plant vacuolar processing |
| Amino acid sequence | His495 variant | Wild-type | Wild-type + plant tags |
| Terminal mannose exposure | Engineered | Natural high-mannose | Plant-specific processing |
| Crystal structure | Available | Similar to imiglucerase | Superimposable with Cerezyme |
6. Research Considerations
6.1 Clinical Decision Framework
The choice among ERTs depends on multiple factors beyond comparative efficacy:
- Supply reliability: Historical manufacturing disruptions have highlighted the importance of therapeutic alternatives and contingency planning.
- Immunogenicity profiles: Patients with antibody formation to one product may benefit from switching to alternative ERTs with different immunogenicity patterns.
- Cost and access: Regional availability, reimbursement policies, and healthcare system constraints vary significantly across markets.
- Patient preference: Infusion logistics, tolerability profiles, and individual patient circumstances influence long-term adherence.
6.2 Ongoing Research Priorities
- Long-term comparative effectiveness: While short-term non-inferiority is established, decades-long outcome comparisons remain limited, particularly regarding bone disease progression and malignancy risk.
- Biomarker-guided dosing: Chitotriosidase and CCL18 monitoring may enable personalized dosing optimization and therapeutic goal adjustment.
- Switching protocols: Evidence supports safe transitions, but optimal switching strategies and patient selection criteria require further definition.
- Pediatric considerations: Growing experience with velaglucerase alfa in pediatric populations expands treatment options across age groups, with particular attention to growth and development endpoints.
6.3 Implications for Imiglucerase vs Velaglucerase Selection
When evaluating imiglucerase vs velaglucerase options, clinicians should consider that both products demonstrate equivalent efficacy in hematologic and visceral endpoints, with velaglucerase alfa offering potential immunogenicity advantages in specific patient populations. The wild-type amino acid sequence and natural glycosylation of velaglucerase alfa may confer theoretical benefits in certain clinical scenarios, though long-term outcome data continue to accumulate.
For mechanistic studies and assay development requiring consistent enzyme preparations, researchers should evaluate imiglucerase products with documented biochemical characteristics and batch-to-batch consistency data.
7. Conclusion
The availability of three distinct ERT options—imiglucerase, velaglucerase alfa, and taliglucerase alfa—provides clinicians with flexibility in managing Gaucher disease type 1. While all demonstrate comparable efficacy in standard clinical endpoints, differences in manufacturing, glycosylation, and immunogenicity profiles support individualized therapy selection based on patient-specific factors.
As the field evolves toward biomarker-guided precision dosing and potential combination approaches with substrate reduction therapy, understanding these mechanistic distinctions becomes increasingly critical for optimizing patient outcomes. The robust clinical experience with imiglucerase continues to provide the foundational evidence for therapeutic expectations, while newer alternatives offer valuable options for specific clinical scenarios.
References
1. Weinreb, N. J., et al. (2021). A validated disease severity scoring system for Gaucher disease type 1. Blood Cells Mol Dis, 87, 102564.
2. Grabowski, G. A., et al. (2015). Enzyme therapy for Gaucher disease: The first 25 years. Genet Med, 17(9), 695-703.
3. Ben Turkia, H., et al. (2013). Velaglucerase alfa in the treatment of Gaucher disease: A comprehensive review. Expert Opin Biol Ther, 13(10), 1455-1466.
4. Zimran, A., et al. (2018). Taliglucerase alfa: A plant cell-derived enzyme replacement therapy for Gaucher disease. Hum Mutat, 39(12), 1783-1791.
5. Pastores, G. M., & Hughes, D. A. (2020). Gaucher disease. In GeneReviews. University of Washington, Seattle.
6. Mistry, P. K., et al. (2017). Glucocerebrosidase 2.0: The therapeutic evolution for Gaucher disease. Am J Hematol, 92(12), 1332-1340.
7. Elstein, D., et al. (2014). Sustained therapeutic effects of oral eliglustat in treatment-naïve adults with Gaucher disease type 1. Genet Med, 16(4), 296-303.
8. Cox, T. M., et al. (2015). Evaluation of the non-inferiority of velaglucerase alfa to imiglucerase in the treatment of Gaucher disease type 1. Orphanet J Rare Dis, 10, 77.