Protocol: Therapeutic Evaluation of IVIg in Passive Murine Models of Immune Thrombocytopenia (ITP)
A Standardized Method for Preclinical Assessment of IVIg Efficacy
Abstract
This protocol establishes a passive ITP mouse model to evaluate the therapeutic effects of intravenous immunoglobulin (IVIg). By administering anti-platelet antibodies to induce transient thrombocytopenia that mimics human ITP pathophysiology, researchers can investigate dose-response relationships and temporal dynamics of platelet recovery following IVIg intervention. This model is suitable for pharmacodynamic assessment of IVIg, mechanistic studies, and preclinical screening of novel therapeutic strategies.
ITP mouse model, IVIg dosing in mice, platelet count assay, mwITP induction, IVIg manufacturing standards
1. Reagent Preparation
1.1 Anti-Platelet Antibody Preparation
- Antibody selection: Use anti-CD41 or anti-CD42b monoclonal antibodies (e.g., MWReg30 or Xia.B2 clone) to induce platelet clearance
- Storage: Stock concentration of 1 mg/mL in aliquots at -80°C
- Working solution: Dilute with sterile PBS to 0.1–0.5 mg/mL before use (determine ED₅₀ based on pilot studies)
- Quality control: Avoid freeze-thaw cycles; prepare fresh working solutions for each experiment
1.2 IVIg Material Considerations
Important Notice: The IVIg referenced in this protocol (Creative Biomart Catalog #THP-0108) is a research-grade active pharmaceutical ingredient (API), not a finished drug product. This material is derived from healthy human plasma via Cohn fractionation with reported endotoxin levels <0.001 EU/μg.
Laboratory Processing Requirements:
- Research-grade IVIg API requires appropriate validation and processing before in vivo use
- Researchers should perform independent quality verification including:
- Sterile filtration and endotoxin testing
- Protein concentration standardization
- Purity confirmation (SDS-PAGE or HPLC per manufacturing guidelines)
- Final formulation must be compatible with murine physiology (isotonic, pH 7.0–7.4)
- Do not assume direct usability without laboratory processing
Physicochemical properties: Molecular weight ~142.7 kDa; complete IgG subclass distribution (IgG1 70.3%, IgG2 24.7%, IgG3 3.1%, IgG4 1.9%)
Working concentration: Adjust to 10–20 mg/mL final concentration based on dosing requirements
Critical: Protein solutions may adsorb to filters; use low-protein-binding filters if filtration is necessary.
2. ITP Model Induction
2.1 Experimental Animals
- Strain: C57BL/6J or BALB/c mice, 6–8 weeks old, mixed gender
- Weight: 18–22 g
- Acclimation: Minimum 1 week in SPF facility
- Group sizes: ≥8 mice per group, including normal control, model control, and IVIg treatment groups (multiple doses)
2.2 Antibody Administration
- Route: Intraperitoneal (IP) injection
- Recommended dose: 2–4 μg/g body weight (based on MWReg30 antibody)
- Injection volume: 5–10 mL/kg body weight
- Induction timing: Day 0 (baseline)
Procedure:
- Weigh mice and calculate antibody amount
- Inject anti-platelet antibody IP (slowly)
- Gently massage injection site to promote absorption
- Record exact injection time
Expected effect: Platelet counts begin declining 2–4 hours post-injection, reach nadir at 6–12 hours (<20% of baseline), and remain low for 24–48 hours.
3. IVIg Treatment Protocol
3.1 Administration Strategy
Use laboratory-processed research-grade IVIg for intervention studies. The IgG subclass profile should approximate human physiological distribution.
3.2 Dose Selection
| Dose Group | Amount | Research Application |
|---|---|---|
| Low dose | 0.5 g/kg | Dose-ranging studies |
| Standard dose | 1 g/kg | Standard therapeutic evaluation |
| High dose | 2 g/kg | Maximal effect studies |
3.3 Administration Routes
- IV injection: Tail vein injection, 100% bioavailability
- Infusion rate: 100–200 μL/min
- IP injection: Alternative for simpler handling
- Dose adjustment: Increase by 10–20% compared to IV route
Tail vein injection is recommended as the standard route for dose accuracy.
3.4 Administration Timing
- Therapeutic administration: 24 hours post-antibody injection (at platelet nadir)
- Prophylactic administration: 2 hours pre-antibody injection (for mechanistic studies)
- Multiple dosing: Repeat at 24-hour intervals for 1–2 additional doses if prolonged effect is needed
4. Assessment Parameters and Blood Collection
4.1 Blood Collection Timepoints
| Timepoint | Relative Time | Purpose |
|---|---|---|
| T₀ | Pre-antibody | Baseline |
| T₆h | 6h post-antibody | Confirm platelet nadir |
| T₂₄h | 24h post-antibody | Pre-treatment level |
| T₃₀h | 6h post-IVIg | Early treatment effect |
| T₄₈h | 24h post-IVIg | Peak effect |
| T₇₂h | 48h post-IVIg | Sustained response |
4.2 Platelet Counting Methods
Method 1: Hematology Analyzer (Recommended)
- Instrument: Sysmex XP-300 or equivalent
- Mode: Murine-specific settings or manually adjusted thresholds
- QC: Daily calibration with control materials
Method 2: Flow Cytometry
- Antibodies: anti-CD41-PE or anti-CD61-FITC
- Internal standard: Fluorescent beads (known concentration)
- Formula: Platelet count (×10⁹/L) = (platelet events/bead events) × bead concentration × dilution factor
Method 3: Manual Counting (Backup)
- Reagent: 1% ammonium oxalate
- Dilution: 1:100 or 1:200
- Count using hemocytometer
5. Expected Results and Data Analysis
5.1 Typical Platelet Recovery Curve
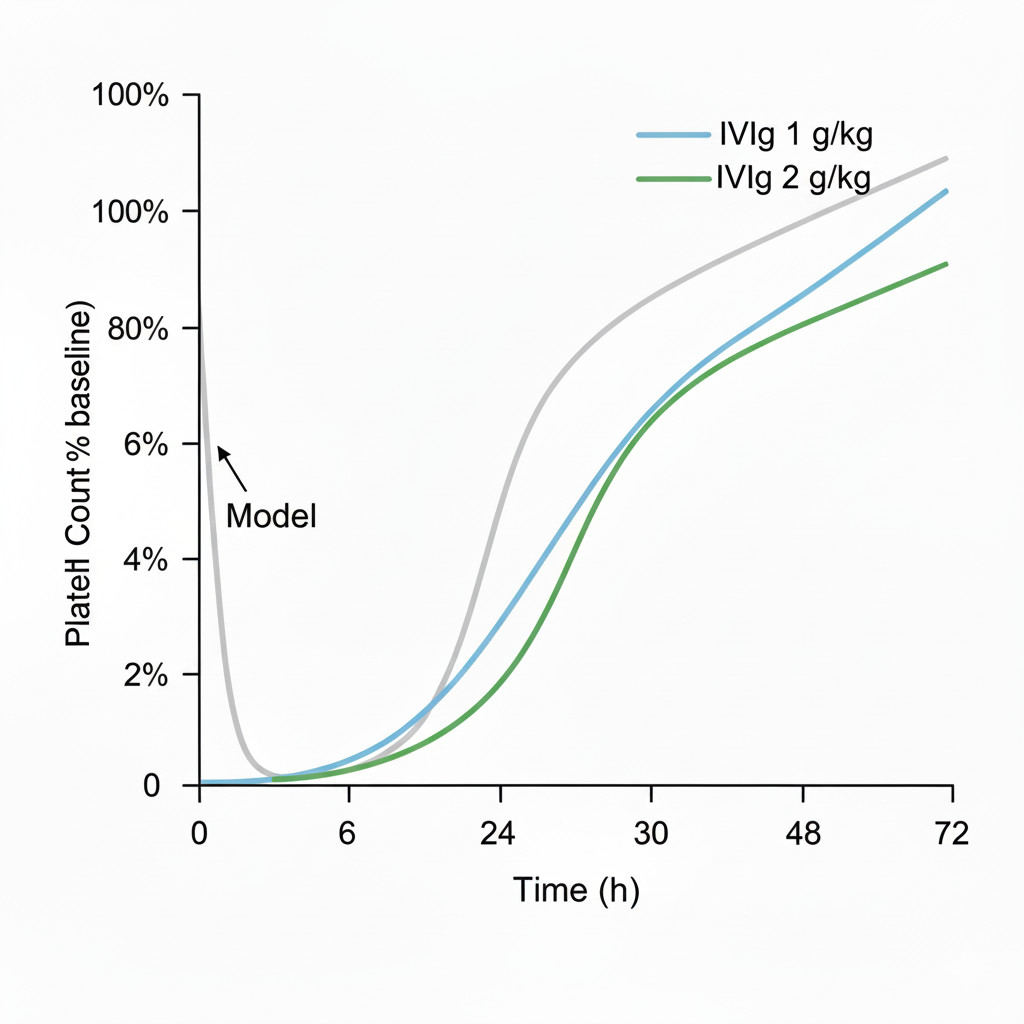
Fig 1. Representative platelet recovery curve in IVIg-treated ITP mouse model (schematic)
Key curve characteristics:
- Model group: Platelets remain <30% of baseline for >48 hours
- Treatment group: Recovery begins at 6h, reaches 50–70% by 48h (1 g/kg)
- Dose-response: Positive correlation between dose and recovery rate/peak
5.2 Statistical Analysis
- Software: GraphPad Prism 8.0 or higher
- Method: Two-way ANOVA with Bonferroni post-test
- Data presentation: Absolute counts, percentage of baseline, AUC analysis
- Significance threshold: *p<0.05, **p<0.01, ***p<0.001
6. Critical Considerations
6.1 Raw Material Quality Control
- Each batch of research-grade IVIg API requires independent quality testing
- Aliquot to avoid freeze-thaw cycles; prepare single-use aliquots
- Animal studies must comply with institutional GLP standards
6.2 Technical Considerations
- Warm tail veins with 37°C water bath before IV injection
- Apply pressure after blood collection to prevent hematoma
- Include age- and gender-matched controls
6.3 Animal Welfare
- Monitor for bleeding symptoms (petechiae, mucosal bleeding)
- Implement humane endpoints if weight loss >15% or activity markedly decreases
- Standard experimental endpoint is 72 hours
References
1. Aslam R et al. Validation of a murine passive ITP model. Platelets. 2019;30(3): 285-294.
2. Crow AR, Lazarus AH. IVIg mechanisms in autoimmunity. Blood Rev. 2018;32(4): 255-263.
3. Nimmerjahn F, Ravetch JV. Immunomodulatory actions of IVIg. Nat Rev Immunol. 2020;20(8): 499-510.
This protocol is provided for research guidance only. Investigators using IVIg active pharmaceutical ingredients must independently validate all materials and procedures. References to commercial products are for informational purposes only and do not constitute usage recommendations or quality guarantees.