From Replacement Therapy to Immunomodulation: The Historical Evolution of IVIg and Its Impact on Modern Drug Discovery
The Transformative Journey from Antibody Replacement to Precision Immunotherapy
Abstract
Intravenous immunoglobulin (IVIg) represents one of the most transformative drug repurposing stories in modern medicine, evolving from a simple antibody replacement therapy to a sophisticated immunomodulatory agent. This article systematically traces the historical trajectory of **[IVIg therapy](/intravenous-immunoglobulin-ivig.html)** from its origins in 1950s plasma fractionation through the pivotal 1981 Imbach ITP study that revealed its immunomodulatory potential, to its current status as a mainstay treatment for over 50 autoimmune and inflammatory conditions. By examining the evolution of plasma fractionation technologies and the clinical paradigm shift initiated by high-dose applications in immune thrombocytopenia (ITP), we elucidate how IVIg's journey has fundamentally reshaped contemporary drug discovery strategies, particularly in Fc receptor-targeted therapeutics.
History of IVIg therapy, Imbach 1981 ITP study, off-label use of IVIg, evolution of plasma fractionation, Fc receptor biology
Fig 1. Historical overview of IVIg's transformation from replacement therapy to immunomodulation
1. Introduction: The Accidental Discovery of Immunomodulation
The story of intravenous immunoglobulin (IVIg) is a testament to clinical serendipity meeting scientific rigor. Originally conceived as a replacement therapy for congenital immunodeficiency disorders, **[IVIg products](/intravenous-immunoglobulin-ivig.html)** have become indispensable tools across neurology, dermatology, hematology, and rheumatology. This transformation was not born from targeted molecular design but from a chance observation in 1981 that forever altered our understanding of antibody therapeutics. Understanding this evolution provides critical insights into how modern drug discovery can leverage clinical observations to unlock hidden mechanisms of existing therapies.
2. Historical Evolution: Three Defining Eras
2.1 The Replacement Era (1950s-1970s): Antibody Supplementation for PID
Technical Foundations: The Cohn Fractionation Revolution
The industrial-scale production of human immunoglobulin began in 1946 with Edwin Cohn's landmark cold ethanol fractionation method at Harvard University. This Cohn fractionation process enabled the first large-scale separation of plasma proteins, with Fraction II+III containing crude IgG that would become the cornerstone of immunodeficiency treatment.
Clinical Application Framework
Following Bruton's 1952 identification of X-linked agammaglobulinemia (XLA), the therapeutic logic was straightforward:
Critical Limitations
Early intramuscular immunoglobulin (IMIg) formulations were painful, poorly absorbed, and volume-limited. The development of acid-treated, pepsin-digested IVIg formulations in the late 1970s solved infusion safety issues but maintained the narrow "replacement" paradigm. The technology focused on preventing aggregation and ensuring pathogen safety, with no consideration for immunomodulatory potential.
2.2 The 1981 Paradigm Shift: Imbach's ITP Revelation
The Seminal Clinical Observation
In a Swiss pediatric ward, Paul Imbach administered high-dose **[IVIg](/intravenous-immunoglobulin-ivig.html)** (0.4 g/kg/day × 5 days) to a child with refractory immune thrombocytopenia (ITP), expecting no benefit—the patient had functional antibodies but was destroying their own platelets. Within days, platelet counts surged from 10,000 to 200,000/μL, a result incompatible with simple antibody replacement.
The Landmark Publication
Imbach's 1981 randomized controlled trial in children with acute ITP demonstrated:
High-dose IVIg (1-2 g/kg) functions as an immunomodulatory drug, not merely a supplement, by saturating Fcγ receptors and neutralizing pathogenic autoantibodies through anti-idiotypic mechanisms.
This Imbach 1981 ITP study fundamentally redefined **IVIg therapy** as a multi-target immunomodulator, triggering exponential growth in production—from <1 ton globally in 1980 to >200 tons today.
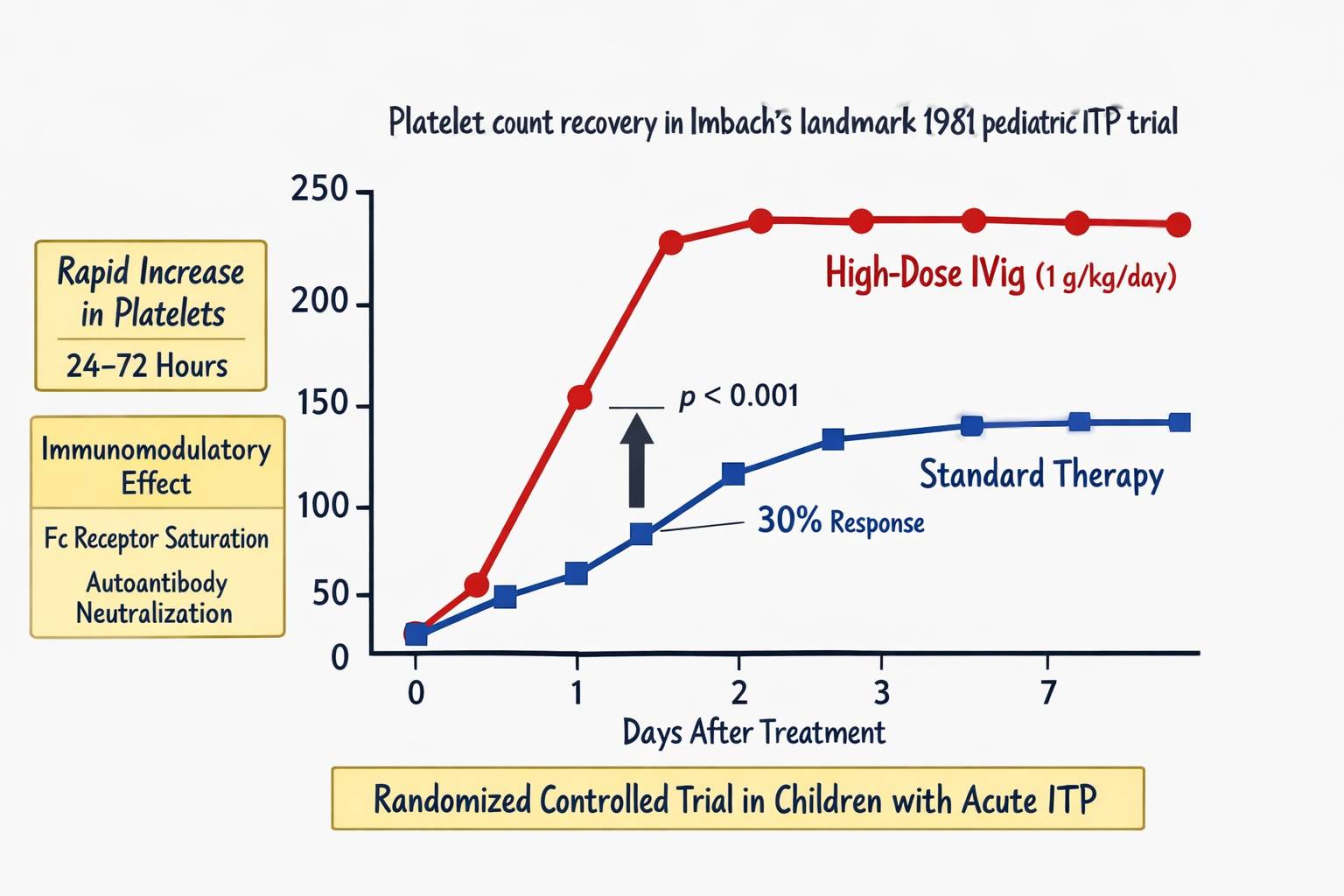
Fig 2. Platelet count recovery in Imbach's landmark 1981 pediatric ITP trial
2.3 Modern Multi-Indication Expansion (1985-Present)
Neurological Applications
| Indication | Approval Year | Key Mechanism | Dose Regimen |
|---|---|---|---|
| Guillain-Barré Syndrome (GBS) | 1985 | Complement inhibition, anti-idiotypic neutralization | 2 g/kg over 5 days |
| Chronic Inflammatory Demyelinating Polyradiculoneuropathy (CIDP) | 1992 | FcγRIIB upregulation, cytokine modulation | 1-2 g/kg/month maintenance |
| Multifocal Motor Neuropathy (MMN) | 1997 | Anti-GM1 antibody neutralization | 2 g/kg/month |
| Refractory Myasthenia Gravis | 2000 (off-label) | FcRn saturation, AChR antibody clearance | 2 g/kg over 2-5 days |
Dermatological and Systemic Applications
Off-Label Use Landscape
The extensive off-label use of IVIg reflects its broad immunomodulatory spectrum, with applications in adult Still's disease, autoimmune encephalitis, and toxic epidermal necrolysis.
3. Mechanistic Dissection: From Clinical Effect to Molecular Target
3.1 Multi-Level Immunomodulation
Modern research has decoded IVIg's complex mechanisms:
4. Implications for Modern Drug Discovery: The Fc Receptor Revolution
4.1 From "Black Box" to Precision Engineering
The evolution of plasma fractionation from Cohn's ethanol precipitation to modern chromatographic methods mirrors the clinical evolution from replacement to modulation. This dual progression informs three critical drug development strategies:
Strategy 1: Deconstructing IVIg into Targeted Biologics
The pharmaceutical industry is "reverse-engineering" IVIg to create precision therapies:
| Drug Class | Mechanism | Development Stage | IVIg Component Mimicked |
|---|---|---|---|
| FcRn Antagonists (Efgartigimod, Rozanolixizumab) | Block IgG recycling | FDA-approved (2021-2023) | FcRn competition |
| FcγRIIB Agonists (SM101) | Activate inhibitory receptor | Phase II | FcγR modulation |
| Engineered IgG1 Fc (M254) | Enhanced FcRn binding | Phase III | Half-life extension |
| Sialylated IgG Fragments | Anti-inflammatory glycoform | Preclinical | Selective anti-inflammatory activity |
Strategy 2: Clinical Observation as Discovery Engine
Imbach's breakthrough exemplifies how off-label use of IVIg can reveal novel mechanisms. Modern drug discovery must:
Strategy 3: Manufacturing Innovation Drives Therapeutic Innovation
The evolution of plasma fractionation technologies has enabled purity improvement from 85% monomeric IgG (Cohn) to >99% (Protein A + SEC), advanced viral clearance, and batch-to-batch CV <5% for critical quality attributes.
4.2 Fc Receptor Biology: The Next Frontier
The success of IVIg has catalyzed intensive research into Fc receptors:
FcγR Family as Therapeutic Targets
FcRn as a Master Regulator
Modern drug discovery has shifted from viewing Fc receptors as passive binding sites to recognizing them as dynamic signaling hubs amenable to pharmacological modulation, a paradigm shift directly stemming from IVIg's clinical mysteries.
5. Conclusion: Balancing Complexity and Simplicity in Drug Development
The history of IVIg therapy teaches that transformative medicines often emerge from the intersection of empirical observation and mechanistic curiosity. From Cohn's centrifuge to CRISPR-engineered Fc variants, the IVIg narrative reveals three enduring principles:
Future Outlook
As FcRn inhibitors and FcγR-selective biologics mature, IVIg may eventually be supplanted in some indications. However, its role as the "original immunomodulatory biologic" will persist—both as a rescue therapy and as a discovery tool. The future likely holds a hybrid model:
The Imbach 1981 ITP study remains a beacon for drug developers: sometimes the most profound therapeutic insights come not from designing new molecules, but from listening carefully to what existing therapies whisper at high doses.
References
1. Imbach, P., et al. (1981). Intravenous immunoglobulin for idiopathic thrombocytopenic purpura in childhood. Lancet, 1(8232), 1228-1231.
2. Cohn, E. J., et al. (1946). Preparation and properties of serum and plasma proteins. J Am Chem Soc, 68(3), 459-475.
3. Schwab, I., & Nimmerjahn, F. (2013). Intravenous immunoglobulin therapy: How does IgG modulate the immune system? Nat Rev Immunol, 13(3), 176-189.
4. Lonberg, N., et al. (2021). FcRn antagonism: A mechanism-based therapeutic approach. Nat Rev Drug Discov, 20(5), 377-398.
5. European Medicines Agency. (2020). Guideline on the clinical investigation of IVIg for off-label use. EMA/CHMP/BPWP/94038/2007 Rev. 3.