Beyond Plasma: Are Recombinant Fc Fragments and Fc-Mimetics the Future of IVIg Therapy?
Evaluating the Competitive Landscape Between Emerging Recombinant Alternatives and Traditional Immunoglobulin Therapy
Abstract
The global plasma supply shortage and escalating costs of intravenous immunoglobulin (IVIg) therapy have catalyzed rapid development of recombinant alternatives, including Fc multimers and FcRn inhibitors. While these engineered therapeutics offer manufacturing advantages and promising clinical results in specific autoimmune indications, they face fundamental biological limitations in replicating the polyspecificity and native glycosylation patterns of plasma-derived IVIg. This analysis examines the competitive landscape between emerging Fc-mimetics and traditional IVIg, evaluating whether recombinant technologies can truly replace or merely complement the current gold standard in immunoglobulin therapy.
Recombinant IVIg alternatives, Fc-mimetics development, FcRn inhibitors, plasma supply shortage solutions, polyspecific immunoglobulin
1. Introduction: The Plasma Supply Crisis Driving Innovation
Intravenous immunoglobulin represents one of modern medicine's most versatile biologics, serving as the standard of care for primary immunodeficiencies, autoimmune neuropathies, Kawasaki disease, and numerous inflammatory conditions. However, this critical therapeutic class faces existential vulnerabilities rooted in its manufacturing paradigm.
The Supply Concentration Risk. Approximately 70% of global plasma collections occur in the United States, creating a geopolitically and logistically fragile supply chain. The COVID-19 pandemic exposed these vulnerabilities when U.S. plasma donations declined by over 20%, triggering worldwide IVIg shortages and forcing treatment rationing across healthcare systems.
The Economic Burden. The complexity of plasma fractionation—encompassing donor screening, viral inactivation, multi-step purification, and rigorous quality control—drives annual treatment costs to $30,000-$100,000+ per patient. This financial barrier disproportionately affects patients in lower-resource regions, creating global inequities in access to essential immunotherapy.
These converging pressures have accelerated investment in recombinant Fc-based therapeutics designed to bypass plasma dependence entirely while potentially offering superior pharmacokinetic profiles and reduced immunogenicity risks.
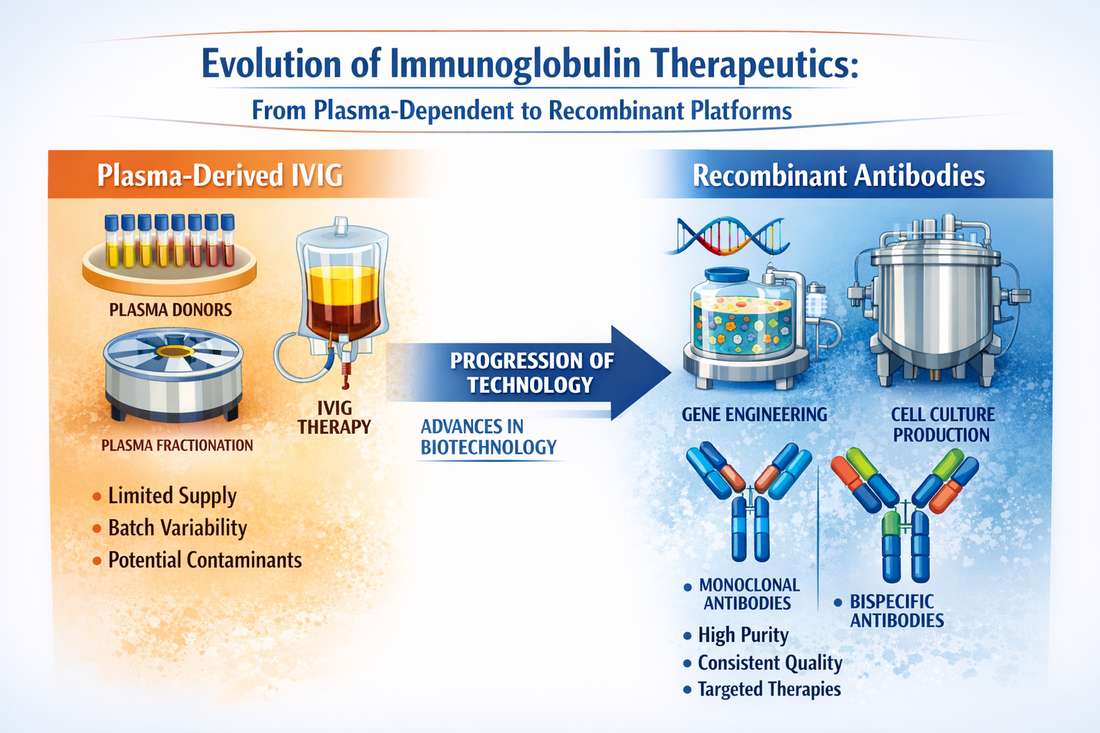
Fig 1. Evolution of immunoglobulin therapeutics from plasma-dependent to recombinant platforms
2. Emerging Competitors: Recombinant Fc Technologies
The current pipeline of IVIg alternatives centers on two distinct mechanistic approaches, both leveraging recombinant protein engineering to manipulate IgG homeostasis.
2.1 FcRn Inhibitors: Accelerating Pathogenic Antibody Clearance
The neonatal Fc receptor (FcRn) serves as the primary regulator of IgG half-life, protecting antibodies from lysosomal degradation through pH-dependent recycling. Blocking this interaction offers a rational mechanism for depleting disease-causing immunoglobulins.
Efgartigimod (Vyvgart) leads this therapeutic class. As a soluble Fc fragment engineered for high-affinity FcRn binding, efgartigimod creates competitive inhibition that accelerates catabolism of endogenous IgG, including pathogenic autoantibodies. Phase 3 trials in generalized myasthenia gravis (gMG) demonstrated rapid, durable responses with subcutaneous dosing schedules superior to conventional IVIg administration.
Rozanolixizumab and nipocalimab (M281) represent additional FcRn-targeting antibodies in late-stage development, each offering distinct binding kinetics and administration routes. These agents collectively demonstrate that FcRn blockade can achieve therapeutic endpoints comparable to or exceeding IVIg in IgG-mediated autoimmune diseases.
2.2 Recombinant Fc Multimers: Mimicking IVIg's Immunomodulatory Effects
Beyond receptor inhibition, several platforms engineer multivalent Fc constructs designed to replicate the immunomodulatory functions of high-dose IVIg through Fcγ receptor modulation.
M230 (formerly efgartigimod precursor) and similar IgG-derived multimers specifically engage inhibitory FcγRIIb while blocking activating FcγRs, recapitulating the anti-inflammatory signaling cascade triggered by IVIg infusion. These candidates offer manufacturing consistency and defined molecular structures unattainable with plasma-derived products.
Advanced Engineering Platforms. Emerging technologies including synFc fusion proteins, synthetic decoy receptors, and bispecific Fc constructs aim to enhance tissue penetration and target specificity beyond what natural immunoglobulins achieve.
| Feature | Plasma-Derived IVIg | FcRn Inhibitors | Fc Multimers |
|---|---|---|---|
| Manufacturing | Plasma-dependent | Cell culture | Cell culture |
| Supply Security | Vulnerable | Stable | Stable |
| Polyspecificity | High (10³-10⁴ specificities) | Single target | Limited |
| Glycosylation | Human-native | CHO-derived | CHO-derived |
| Clinical Experience | Decades | Limited | Limited |
| Current Cost | High | Moderate-High | TBD |
Table 1: Comparative analysis of immunoglobulin therapeutic platforms
3. The Irreplaceable Advantages of Natural IVIg
Despite recombinant advances, plasma-derived IVIg products maintain inherent biological properties that current engineering cannot fully replicate.
3.1 Polyspecificity: The Power of Diversity
Natural IVIg contains antibodies derived from thousands of healthy donors, creating an antibody repertoire with extraordinary diversity—estimated at 10³ to 10⁴ distinct specificities. This polyspecificity enables simultaneous neutralization of diverse pathogens, toxins, and autoreactive epitopes. Recombinant Fc therapeutics, by contrast, typically target single mechanisms or limited antigen panels, potentially missing the broad-spectrum immunomodulation that characterizes IVIg efficacy in complex inflammatory conditions.
3.2 Native Glycosylation and Effector Function
The N-linked glycans at IgG's CH2 domain critically modulate FcγR binding, complement activation, and anti-inflammatory activity. Natural IVIg exhibits heterogeneous glycosylation patterns—including specific sialylation and galactosylation profiles—that contribute to its immunoregulatory properties. While CHO cell expression systems can produce glycosylated antibodies, precisely replicating the complex, dynamic glycan profiles of pooled human IgG remains technically challenging.
3.3 Mechanistic Breadth
IVIg therapy operates through multiple concurrent mechanisms:
- Fc-mediated effects: FcγR modulation, complement interference
- Fab-mediated effects: Pathogen and toxin neutralization, idiotype-anti-idiotype networks
- Cellular modulation: Regulatory T-cell expansion, dendritic cell modulation
Recombinant Fc fragments capture only the Fc-dependent functions, while losing the Fab-mediated antigen recognition that contributes to IVIg's efficacy in infectious and idiopathic conditions.
3.4 The Gold Standard Validation
Notably, in head-to-head clinical trials evaluating novel Fc therapeutics, investigators consistently designate plasma-derived IVIg as the active comparator or standard-of-care control. This experimental design choice itself validates IVIg's continued status as the benchmark against which all alternatives must measure.
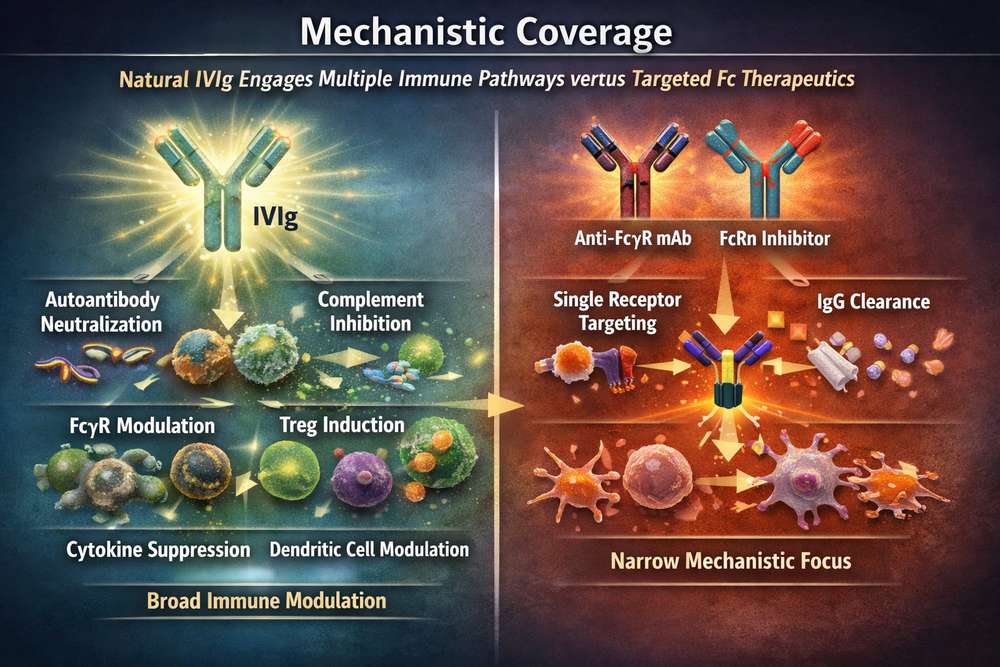
Fig 2. Mechanistic coverage: Natural IVIg engages multiple immune pathways versus targeted Fc therapeutics
4. Clinical Reality: Replacement or Complementation?
The emerging consensus suggests recombinant Fc technologies will not immediately replace IVIg treatment but rather establish complementary roles:
Near-term positioning (2024-2030): FcRn inhibitors and Fc multimers will likely dominate specific IgG-mediated autoimmune indications—particularly myasthenia gravis, CIDP subsets, and ITP—where rapid IgG lowering offers clear mechanistic advantage. These represent addressable markets of $3-5 billion annually.
Persistent IVIg dependence: Primary immunodeficiency, multifocal autoimmune diseases, and off-label inflammatory conditions will continue requiring plasma-derived products due to the need for broad antibody replacement and polyspecific immunomodulation.
Hybrid therapeutic paradigms: Future treatment algorithms may sequence recombinant agents (for rapid disease control) with IVIg (for maintenance and infectious protection), optimizing both efficacy and plasma resource utilization.
5. Conclusion: Toward a Diversified Therapeutic Arsenal
The question "Will recombinant Fc fragments replace IVIg?" may be less relevant than "How will these technologies reshape immunoglobulin therapy?" Current evidence indicates that while IVIg remains the gold standard for comprehensive immunomodulation and antibody replacement, recombinant alternatives are carving essential niches in autoimmune disease management.
True therapeutic innovation lies not in binary replacement but in developing a stratified toolkit: FcRn inhibitors for rapid autoantibody depletion, Fc multimers for targeted immunomodulation, and plasma-derived IVIg for situations requiring biological diversity and comprehensive immune support. This diversified approach promises enhanced patient access, reduced supply vulnerability, and ultimately, precision immunotherapy tailored to specific disease mechanisms.
The future of immunoglobulin therapy extends beyond plasma—but it does not leave plasma behind. The convergence of recombinant engineering and plasma-derived biologicals will define the next era of immunomodulatory treatment.
References
1. Cohn EJ, et al. (1946). Preparation and properties of serum and plasma proteins. IV. A system for the separation into fractions of the protein and lipoprotein components of biological tissues and fluids. Journal of the American Chemical Society, 68(3), 459-475.
2. Howard JF Jr, et al. (2017). Safety and efficacy of eculizumab in anti-acetylcholine receptor antibody-positive refractory generalised myasthenia gravis (REGAIN): a phase 3, randomised, double-blind, placebo-controlled, multicentre study. The Lancet Neurology, 16(12), 976-986.
3. Ulrichts P, et al. (2018). Neonatal Fc receptor antagonist efgartigimod safely and sustainably reduces IgGs in humans. The Journal of Clinical Investigation, 128(10), 4372-4386.
4. Guo Y, et al. (2022). FcRn antagonism as a therapeutic strategy for autoimmune diseases. Frontiers in Immunology, 13, 891234.
5. Schwab I, Nimmerjahn F. (2013). Intravenous immunoglobulin therapy: how does IgG modulate the immune system? Nature Reviews Immunology, 13(3), 176-189.